
🧵on the Imperial study on omicron severity TL;DR:
-*intrinsic* omicron severity similar/bit lower to delta
-*observed* severity lower due to omicron more likely to re-infect
-vaccine efficacy against hosps maintained
-growth rate likely to override impact of lower severity
-*intrinsic* omicron severity similar/bit lower to delta
-*observed* severity lower due to omicron more likely to re-infect
-vaccine efficacy against hosps maintained
-growth rate likely to override impact of lower severity
Before I get into the rest, I want to re-emphasise that the overall impact of omicron will be determined by growth (exponential) and severity (linear)- even with lower severity, growth in itself will cause serious impact at population level, even if severity is moderately lower.
The Imperial study is a complex piece of analysis, and I have to commend the Imperial team for dealing with important confounders in the analysis.
I want to first explain this a bit more.
I want to first explain this a bit more.
I want to first separate out *intrinsic severity* of omicron relative to delta from *observed severity*. This distinction is important - because it separates the instrinsic properties of the virus from differences in severity because of who it infects.
By intrinsic severity, I mean if omicron was introduced into the same people as delta, what would the relative severity be?
By observed severity, I mean what is the observed (real-world) severity of omicron infections relative to delta infections?
By observed severity, I mean what is the observed (real-world) severity of omicron infections relative to delta infections?
What determines the severity of an infection?
-age
-gender
-ethnicity
-socio-economic status (proxy for several other factors)
-past infection
-vaccination
-age
-gender
-ethnicity
-socio-economic status (proxy for several other factors)
-past infection
-vaccination
So differences in severity between variants can be down to:
-differences in ages/genders of those infected
-differences in demographic factors (e.g. region/deprivation)
-differences in vaccination status
-previous infection status
-differences in ages/genders of those infected
-differences in demographic factors (e.g. region/deprivation)
-differences in vaccination status
-previous infection status
This is vitally important to consider when comparing omicron to delta because delta & omicron infections are occurring in different groups. e.g. For omicron 13% of cases have had previous infection >90 days ago (so are defined as re-infections), compared to only 2.5% for delta.
This is of course consistent with significant immune escape of omicron relative to delta, which is clearly contributing to its advantage in growth over delta. But of course previous infection may also provide protection against severe disease reducing *observed severity*.
This is very likely at least a major part of the reason why the current wave in SA seems to be associated with a much lower hospitalisation rate than the 3rd wave - because many people were infected in the 3rd wave and much larger population had been exposed to infection before.
The problem is we don't really have good data on previous infections. The total infections that have occurred are likely several times higher than those reported. Pillar 2 (community tests) show only 17% of the population was infected so far. True infection is likely much higher.
The analysis essentially compared hospitalisation risk between omicron and delta among people who tested PCR positive between 1st and 14th December 2021 - comparing hospitalisation rates between SGTF -ve (good proxy for omicron) and SGTF +ve (good proxy for delta cases).
It adjusted for age, sex, ethnicity, region & specimen date, and presented the risk of hospitalisation for omicron *relative to* delta by vaccination status.
To try and understand *intrinsic severity* of omicron relative to delta, the authors tried to account for past infection as well. This is because past infection would make a big difference to estimates, given that omicron is associated with much higher re-infection that delta
The problem as stated before in re-infection is likely hugely underestimated, simply because first infections are hugely underestimated (because only a small proportion test, and are reported overall). They assumed that only 1/3rd of all re-infections had been identified.
With this assumption, they were able to then correct *observed* estimates (which would be affected by level of past infection & immunity) to get a less skewed estimate of *intrinsic severity*. The corrected estimates are more likely to give us an idea of intrinsic severity.
But these do depend on the assumptions made (about the level of underestimation of re-infection), so have to be taken with that caveat. Based on this, 40% of omicron cases were assumed to be re-infections, and ~8% of delta infections (3x observed percentages). 
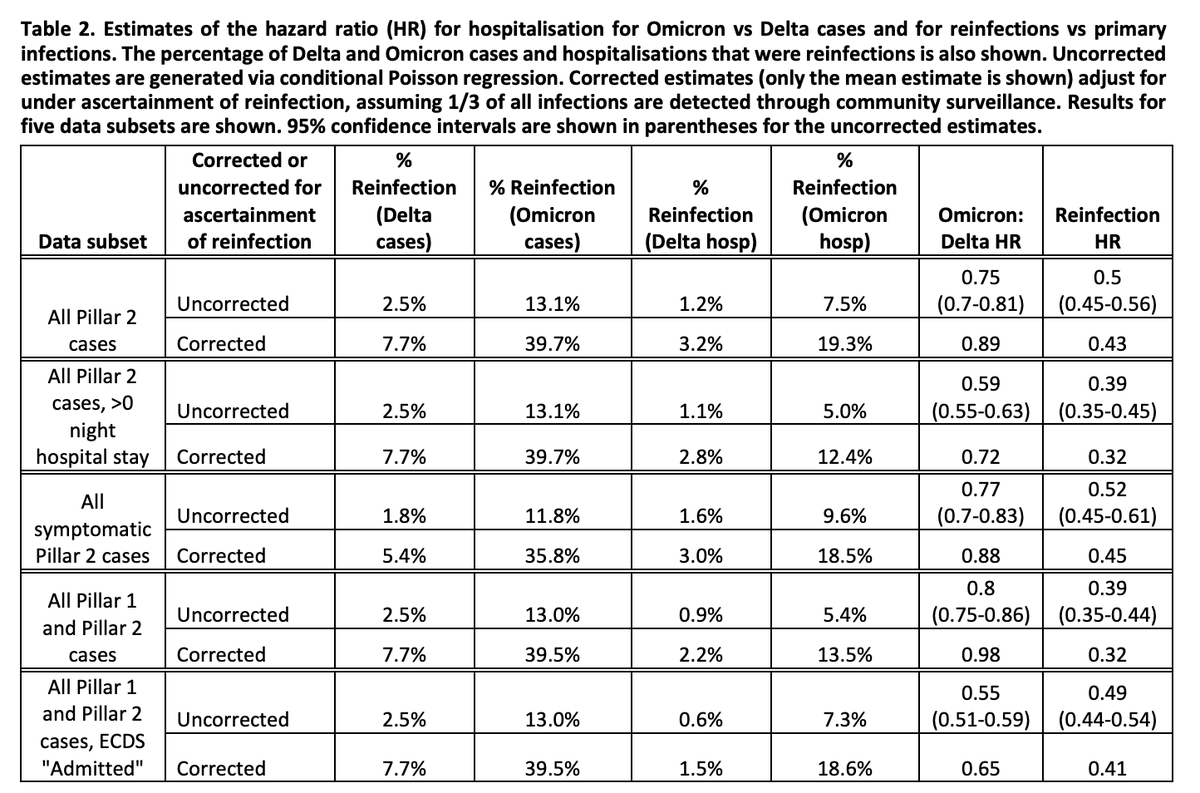
Assuming this, they found that omicron had only very slightly reduced risk of hospitalisation relative to delta -0-30% in different analysis, but protection from hospitalisation for re-infections was ~55-70% for omicron.
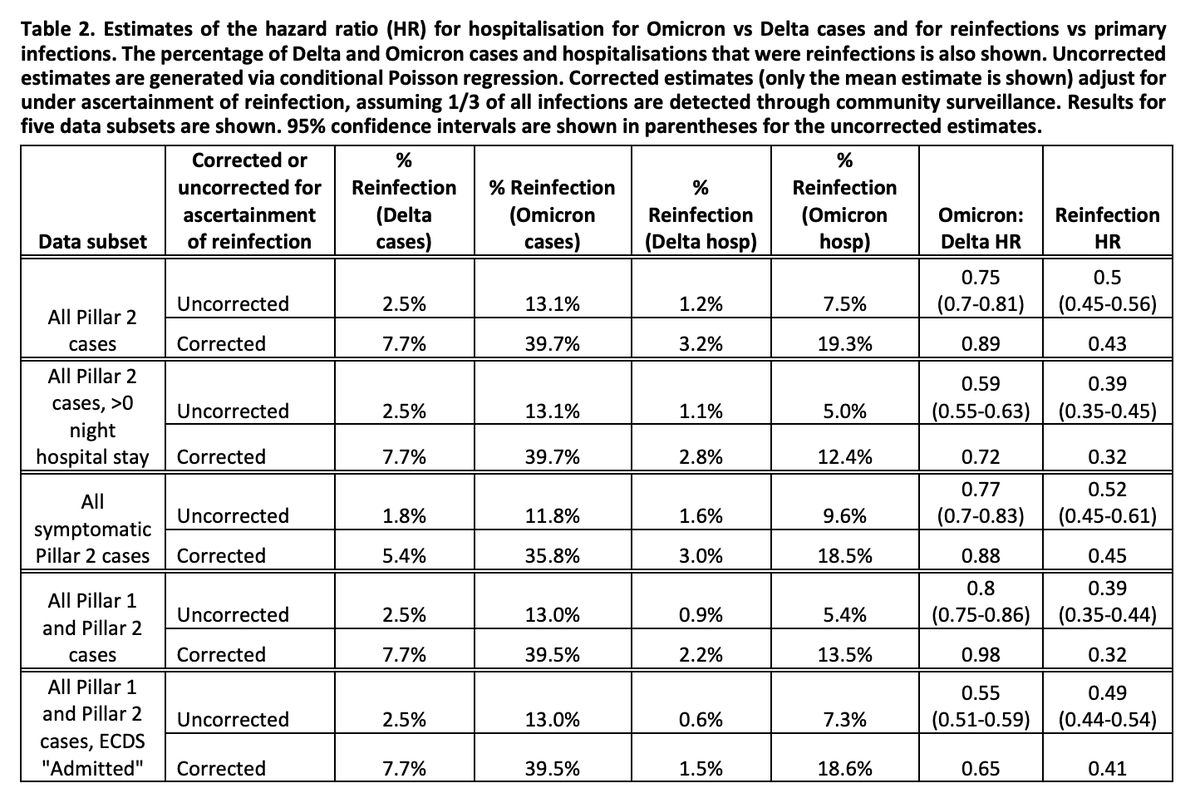
Remember that while this means similar *intrinsic severity*, overall real observed severity is reduced compared to delta simply because omicron has 40% of cases that are re-infections (who are more protected than those that are 1st infection) compared with delta.
When we don't consider underestimation of re-infections then *intrinsic severity* is reduced by 15-20% and reinfection is estimated to be associated with approximately a 50-60% reduction in hospitalisations.
Overall, the findings are not hugely different regardless of assumptions. All suggesting that observed reduction in severity is very likely due to the fact that a much larger proportion of omicron cases are people with prior infection - so greater protection.
So not much difference due to the intrinsic properties of the virus - but rather who it's infecting. Remember the comparisons so far were adjusted for vaccine status, so were only comparing impact *within* compartments of different levels of vaccination, & averaged across these.
What does the study tell us about vaccine efficacy?
We can look at the same data but by vaccine status, adjusting for all the other factors. Remember that these estimates are presented as protection against hospitalisation *once* infected, so don't account for total protection
We can look at the same data but by vaccine status, adjusting for all the other factors. Remember that these estimates are presented as protection against hospitalisation *once* infected, so don't account for total protection
Total effectiveness is protection from infection *and* protection from hospitalisation. Here we're only looking at the 2nd. The study shows that *if infected* efficacy in preventing severe disease for 2 doses AZ for omicron is 60-70% compared to an unvaccinated person with delta.
And protection *if infected* with omicron with 2 doses Pfizer is ~80% *relative to* delta infection in unvaccinated. With boosters (AZ/Pfizer/Moderna) efficacy is 70-80%. Overall, the effectiveness of omicron against severity seems to be similar to delta across all vaccines.
Ultimately what matters within the UK is probably going to be *observed severity* right now, because this is a combination of all factors- intrinsic severity of the virus + the protections/severity based on who it's infecting.
But intrinsic properties important to understand to generalise to future scenarios, and also other countries. As the authors say ultimately the impact will be determined by growth and severity.
There are also some indicators that hospitalisations with omicron may potentially be shorter duration compared with delta, but it's difficult to know from the current study as on average follow up of omicron cases was shorter.
Growth is rapid and exponential. And this will easily override even moderate reductions in severity. For a variant half as severe as delta, doubling in 2 days would mean the same level of overall hospitalisations just in 2 days due to the large numbers infected.
Ultimately, the growth rate means, despite moderate reductions in severity, hospitals could still be overwhelmed, and we still need to take urgent action to pre-empt this, while we understand more about this threat.
The effectiveness of vaccines holding up against severe disease is a huge relief, but unsure what all this means for long COVID, given effectiveness against infection has been shown to be quite low even with 2 doses with omicron.
Long COVID burden could be significant if protection doesn't hold up with vaccines (certainly seems that it doesn't for infections at least with 2 doses), emphasising the need for a vaccine plus approach to protect people.
Want to add on further insights from reading Nick Davies's really helpful thread this morning:
https://twitter.com/dgurdasani1/status/1473953715954532356?s=20
• • •
Missing some Tweet in this thread? You can try to
force a refresh


