
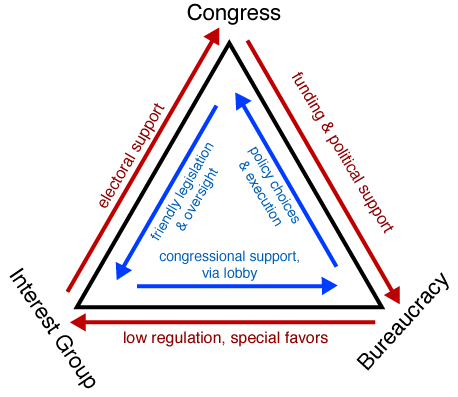
ICYMI people in pain & PWUD have been harassed, endangered, and killed because of poorly designed drug policy. The ivory tower drug war perpetrated by the iron triangle of inept bureaucrats, interests, and Congress has now reached into healthcare targeting our most vulnerable.🧵 
https://twitter.com/LeahabShaffer/status/1475232216548614146
Some love to claim science can fix all our problems but in the case of drug prohibition, which now affects our sickest, those using low/no evidence "science" to justify such policies have already unleashed unprecedented harm on the American people and destroyed population health.
A "vaccine" is not a tool for PWUD to "overcome opioid addiction." Not only does this border on unethical, but it'll also be used to continue justifying deadly policies that now impact sick and injured patients. It's also likely to result in more suicides.
https://twitter.com/LeahabShaffer/status/1475232984575926276
A "vaccine for addiction" that makes drug use more difficult is simply one more path-dependency justified by the unholy trinity of industry, academia, and their friends within government to maintain/increase resources. This has been the status quo for 40 years with awful results.
Your claim that PWUD "need all the tools in the toolbox" to "overcome opioid addiction" using "replacements like methadone, blockers like vivitrol, counseling and healthcare, and antibodies to help out of rehab" is beyond naive. It borders something else entirely.
In fact, your naive claims cross directly into enabling a greedy system that will continue to harm countless American taxpayers. One that kills with impunity. Their interventions using our tax $$$ have made things infinitely WORSE. How long are we expected to bankroll failure?
Your other claims concerning people in pain are similarly naive. CDCs Rx guidelines were not supposed to be weaponized either but they were. I'm sure that isn't the stated goal for this "vaccine" either, but that's exactly what will happen. It'll be exported to pain patients.
Because use is conflated w/abuse. Those of us who pay attention to drug policy know this. Tools and language have & will be weaponized for profit. If you don't recognize the trends after what's transpired in the wake of the CDC "guidelines," then you're NOT paying attention.
How we "treat drugs of abuse" and policy should be simple. #HarmReduction should be employed. Because if we don't? Instead of 100k dead in 1 year, we're going to see a whole lot more. And these are just the deaths we KNOW about. These policies have FAILED repeatedly for decades.
In the wake of the CDC guideline, patients have been rationed out of the healthcare delivery model. How? By building those "guidelines" directly into clinical decisions support & other systems. This is the health IT ecosystem. A system that was built for surveillance & rationing.
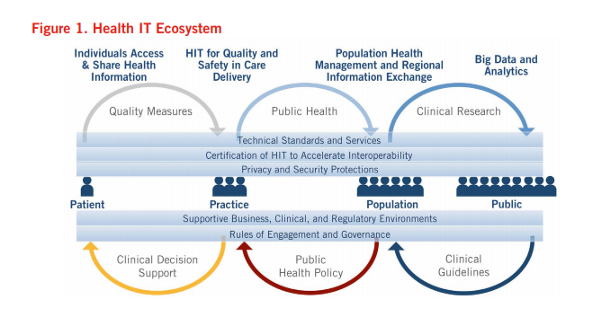
They call this a "learning health system," except it rations out undesirable patients based on immutable characteristics and histories such as (medical/other) drug use. Interoperability and all the rest of it aren't yielding healthier people, better care, or smarter spending.
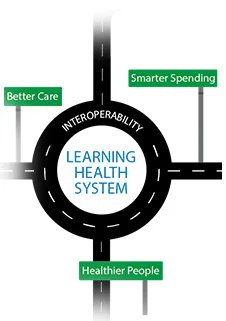
It's yielding poor health outcomes that aren't even being tracked. Those who haven't been rationed out of the system are being studied without their knowledge or consent in many cases (ePCTs & CER), while this system "learns" how to further discriminate & erect barriers to care.
You add something like "opioid vaccine hesitancy" to the list for predictive analytics and we're going to see discrimination and poor health outcomes on a level never before seen in history. Results will be even starker than those seen in the wake of CDCs unscientific guidelines.
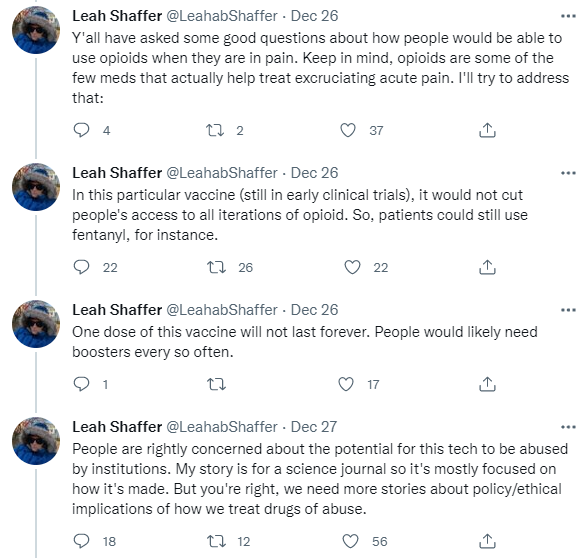
Your claim that an opioid "vaccine" wouldnt "cut into patients access to all iterations of opioids" borders on ridiculous in light of recent history. Your claim that "patients could still use fentanyl" shows your complete lack of knowledge of the current climate/policy landscape.
Maybe you're completely unaware, but pain patients can scarcely access ANY analgesics or even basic primary care now. This includes cancer & hospice patients. We're denied access for fear of "addiction" affecting around 1-3% of the entire population (< than 1% for pain patients).
As a writer, you should already be attuned to these facts. It's much more likely people with chronic health conditions/pain will be the ones pressured to take this "vaccine" on the condition of continued care using modalities that have already been proven largely ineffective.
TLDR
Scientific curiosity has a dark side. An "addiction vaccine" will be leveraged by an out-of-control bureaucracy bent on waging war on Americans. All with help from the National Academy of Sciences (NAS).
Scientific curiosity has a dark side. An "addiction vaccine" will be leveraged by an out-of-control bureaucracy bent on waging war on Americans. All with help from the National Academy of Sciences (NAS).
The NGOs under NAS need to be reigned in after advising our federal government to build this discriminatory "learning health system" that brought this war on people to the doctors office. Their FACA exemptions should also be viewed with the deepest suspicion & legally challenged.
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh





