
OK, quick rundown on the reading I've been doing this morning on booster efficacy and Omicron.
Most of the data we have is from the UK, and most if it isn't exactly garbage, but it is highly contaminated: there is as much noise as signal.
Most of the data we have is from the UK, and most if it isn't exactly garbage, but it is highly contaminated: there is as much noise as signal.
First, to set the stage, the UK has about a 34% booster rate. That *should* give some decent statistical basis for analysis - but it doesn't.
The UK preferentially boostered the at-risk - elderly and immunocompromised.
The UK preferentially boostered the at-risk - elderly and immunocompromised.
That means that their population-level booster stats are going to show more rapid declines than the *actual* population level booster stats - those folks' immune systems don't mount as rigorous a response, nor do they maintain as strong a memory function.
The report is not well done. It elides confounders - doesn't even attempt to identify them, let alone account for them.
It is also very lacking in the methods section, and I haven't had time to dig back into previous reports to completely elucidate all the details. I do follow the basic methodology, though.
Here's the figure that immediately jumped out at me:
Here's the figure that immediately jumped out at me:

They use a negative case control method, which is weaker than an RCT, because the analyst is making decisions about whop should be in the control arm - the retrospective equivalent of the placebo arm in an RCT.
That introduces bias from the jump.
That introduces bias from the jump.
One of the biases is that most people who enter an RCT are relatively self-aware and more cautious than the gen pop.
With case controls, that natural self-selection method is absent. It's been shown in other real world examples in this pandemic, that the vaccinated assume far too much protection. Young, vaccinated people's behavior was far riskier than it should have been.
Go back and look at this figure again. Anything bother you?
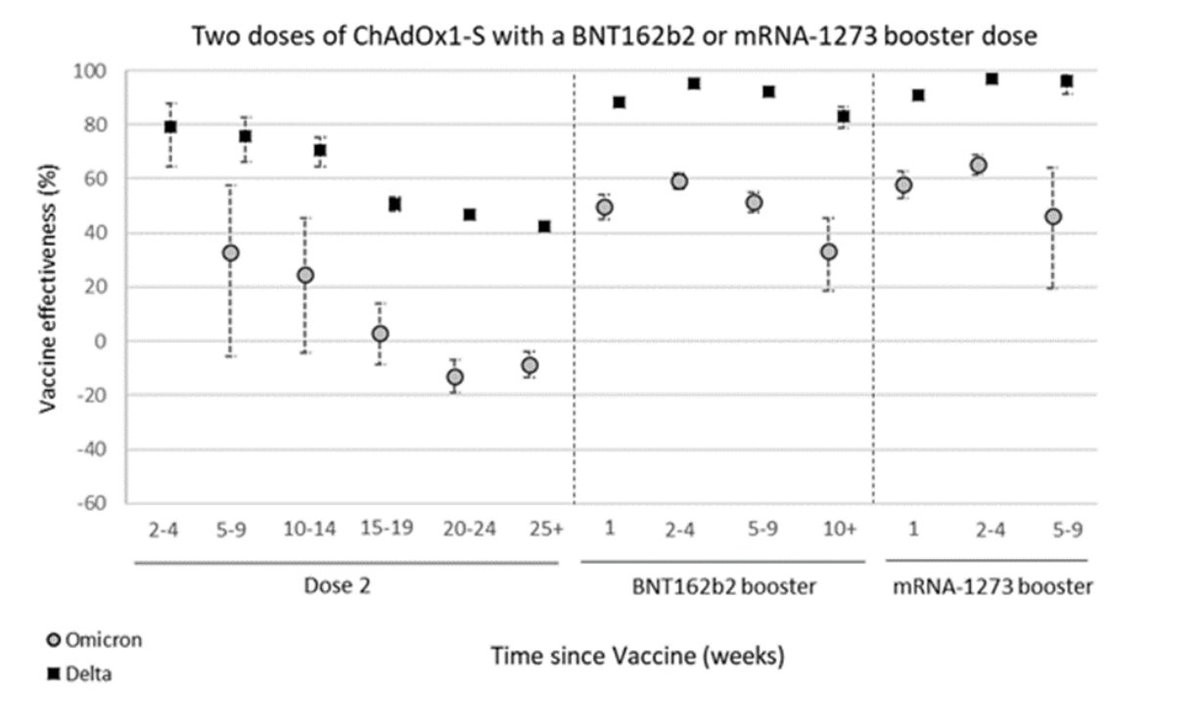
*Negative* protection at 20 weeks sure as fuck bothers me.
Gotta go, will pick up this thread in a few.
Gotta go, will pick up this thread in a few.
OK, back from teaching the sprog to drive. Lost a few years of my life, but it's all good. 😱
The other thing that bothers me is that after dipping below zero, the point estimate for Omicron protection from 2 doses went back up at 25 weeks, with near statistical significance.
The other thing that bothers me is that after dipping below zero, the point estimate for Omicron protection from 2 doses went back up at 25 weeks, with near statistical significance.
That, to me, indicates serious issues with sampling.
Could also be a problem with their case-control algorithm, but they didn't publish that, so I have no idea.
Could also be a problem with their case-control algorithm, but they didn't publish that, so I have no idea.
If we look at another UK study, this time from Scotland, their 2 week efficacy results from boosting are quite different:
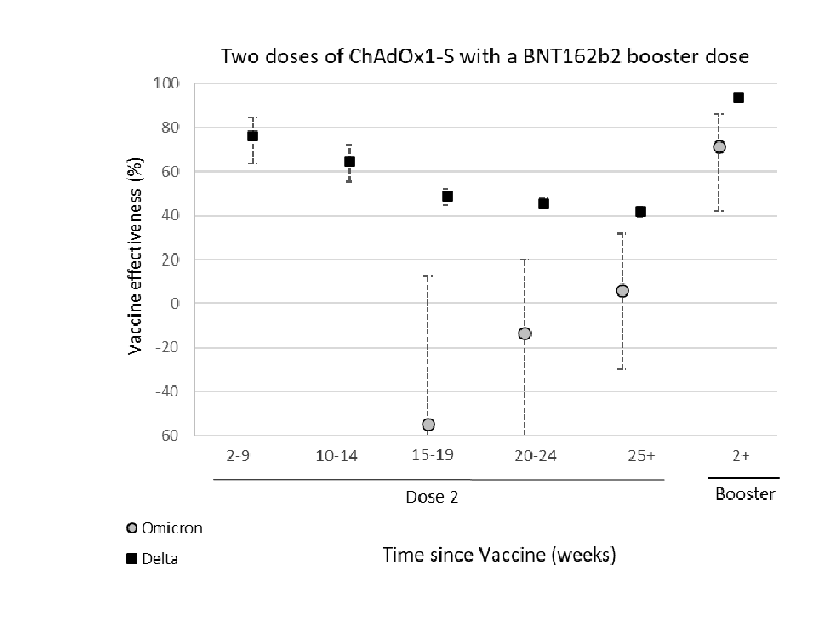
So I'm comparing epi studies in the same country, though different regions, so I should not have too many confounders, and one tells me 2 week efficacy of boost against symptomatic disease with Omicron is 60%, the other than it's 75%.
medrxiv.org/content/10.110…
medrxiv.org/content/10.110…
That kind of variation in similar population once again indicates sampling bias.
Aside from the potential confounders I've already noted, there is one that the UK report did note: Omicron cases are enriched in travelers who will have had a different exposure risk, even IF their behavior was similar.
The more viral particles you breathe in, the lower your vaccine protection against symptomatic disease is going to be.
Another issue is that younger people are less risk-averse, and this data is not age-stratified.
So I don't know if exposure risk was the same for Delta victims in the UK as it is for Omicron. I strongly suspect it isn't.
So I don't know if exposure risk was the same for Delta victims in the UK as it is for Omicron. I strongly suspect it isn't.
I do NOT believe that the broader literature or our real world experience backs up the conclusion that this method comes to: that with Omicron it's worse to have a vaccine than not after 20 weeks.
The fact that the report didn't even attempt to address this issue is a major flaw
The fact that the report didn't even attempt to address this issue is a major flaw
Another issue is shifting populations from “study” to study. So those of you who have read my tweets bitching about meta-analyses (meta analysis is to analysis as metaphysics is to physics) will now get a real world example of why I have that attitude.
This thread gives a really big clue about what at least one of the issues is:
https://twitter.com/DevanSinha/status/1474105593308737540
The “control” group of case negative, unvaccinated, controls is far more likely to have had a prior infection now than in the original vaccine trials. The controls are no longer naive. Probably a third of the controls picked by the UK analysis have some immunity.
Remember that vaccine efficacy calculations are a function of the ratio of people who got COVID while vaccinated to those who didn’t. These aren’t raw, absolute infection numbers. So if you give the unvaxxed an immune boost, the vaccine is going to look relatively worse.
This is likely part of what’s happening, here, along with differential exposure.
So how long *does* the booster protect for?
Beats my pair of jacks.
But the 10 weeks out of the the UK study probably isn’t even the lower bound, given the issues with the data and analysis.
So how long *does* the booster protect for?
Beats my pair of jacks.
But the 10 weeks out of the the UK study probably isn’t even the lower bound, given the issues with the data and analysis.
So, a couple of addenda to describe the data that informs my current personal decisions.
Boosted spike titers shoot up many times higher than after the second dose. It makes no sense that there would be a dropoff to baseline as fast as two months, when the lower titers from the second shot decay much more slowly.
Here's some modeling versus Delta based on increases in titers observed in human subjects post-boost.
The biology just doesn't add up to the UK modeling.
thelancet.com/journals/lanmi…
The biology just doesn't add up to the UK modeling.
thelancet.com/journals/lanmi…
The other question I have is about the definition of "symptomatic disease". That covers a lot of ground from post-nasal drip and a mildly sore throat to the body slam that the second shot gave me to just short of heading to the ER.
I have a suspicion that boosted "symptomatic disease" is a lot milder than unboosted, but that data wasn't collected.
So where does that leave me in my personal risk calculus?
So where does that leave me in my personal risk calculus?
Omicron has so much immune escape potential that I'm back to short, fast trips to the grocery store and take-out only on prepared food.
All of those with N-95s, rather than our home-made HEPA masks I was using last year.
All of those with N-95s, rather than our home-made HEPA masks I was using last year.
With that level of paranoia in mind, I'm not completely relying on the booster to protect me - I'm assisting it by breathing in as few virons as I possibly can.
Given the range of values in the literature for the duration of NAbs, I have a feeling the booster is good for 4 - 6 months.
I'm waiting to see if an Omicron-specific booster comes out, or if one of the intra-nasals is approved. If that happens, I will get those, immediately.
I'm waiting to see if an Omicron-specific booster comes out, or if one of the intra-nasals is approved. If that happens, I will get those, immediately.
Otherwise, I'll wait out to the 5 month mark and look for another original flavor booster. That would mean about April for me.
YMMV, I am not THAT kind of doctor, etc., etc.
As always, these threads are purely to demonstrate what a semi-expert in this field who reads widely and then parses the breadth and depth of the published data is doing with that information on a practical level.
As always, these threads are purely to demonstrate what a semi-expert in this field who reads widely and then parses the breadth and depth of the published data is doing with that information on a practical level.
If you're immunocompromised, most DEFINITELY consult your physician and not my threads.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


