.@tom_cardoso, @globeandmail why are you interviewing ID MDs about Respiratory PPE? Lynora Saxinger has muddied the science of Airborne Transmission and obstructed access to Respiratory PPE for 2 years. She and the other obstructionists are liable. They are not honest brokers. 1/
https://twitter.com/globeandmail/status/1477043405104443393
What training do these MDs have in Respiratory PPE and the physics of masks?
This would be like doing an investigative report on the Boeing 737MAX crashes, and only interviewing the Boeing and FDA executives that rubber stamped the negligent certification documents. 2/
This would be like doing an investigative report on the Boeing 737MAX crashes, and only interviewing the Boeing and FDA executives that rubber stamped the negligent certification documents. 2/
Right off the bat... does this quote not strike you as odd? Have you seen a respirator? They are not individually fit/molded to a person's face. They are DESIGNED to fit, UNLIKE A SURGICAL MASK.
You know what mask forces air out the sides 100% of the time? A SURGICAL MASK. 3/
You know what mask forces air out the sides 100% of the time? A SURGICAL MASK. 3/
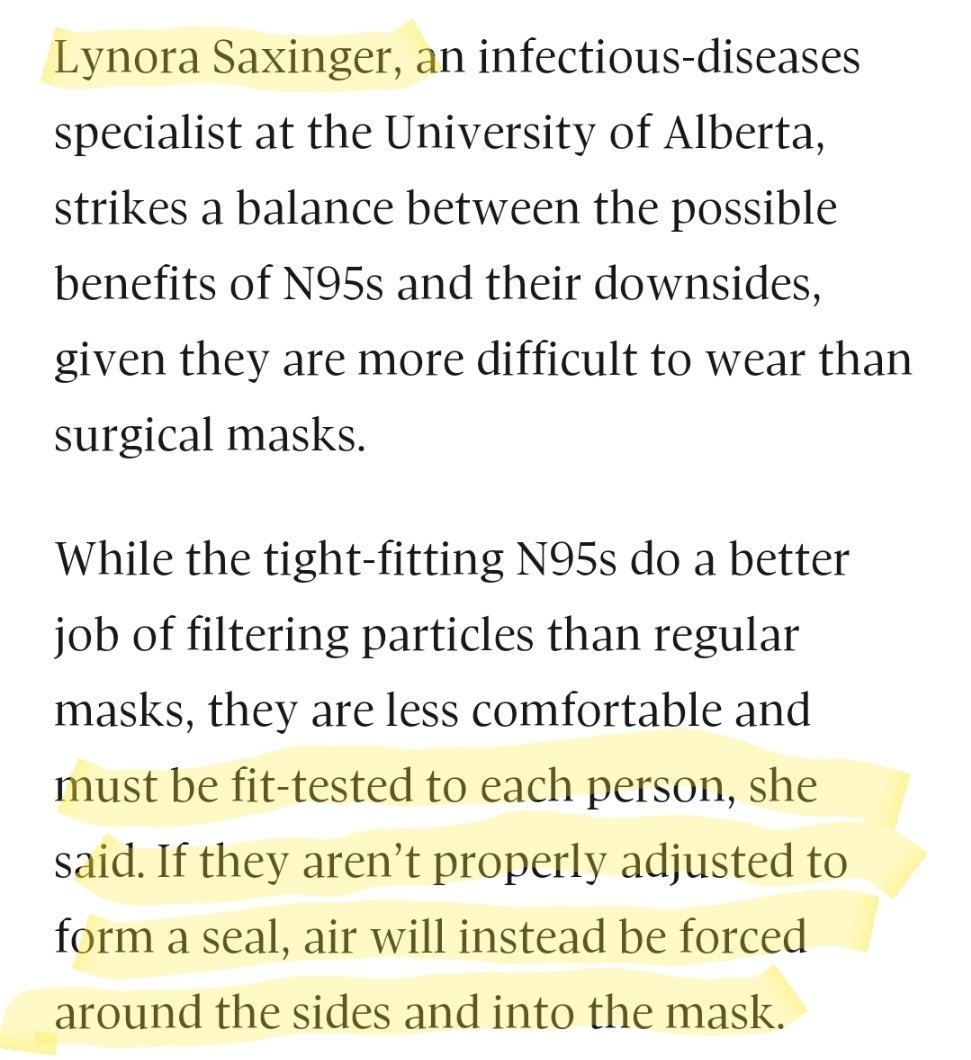
A respirator that fails a fit test, just means it's not achieving optimal protection for an Occupational Hazard.. it's still orders of magnitude better than a surgical mask, WHICH HAS VISIBLE GAPS ALL AROUND IT!
Here's a DIY fit-test, try it yourself.
4/
Here's a DIY fit-test, try it yourself.
4/
https://twitter.com/JenniferKShea/status/1472417124048064519?t=MvuWOOUhKreJ5xD6khZKZw&s=19

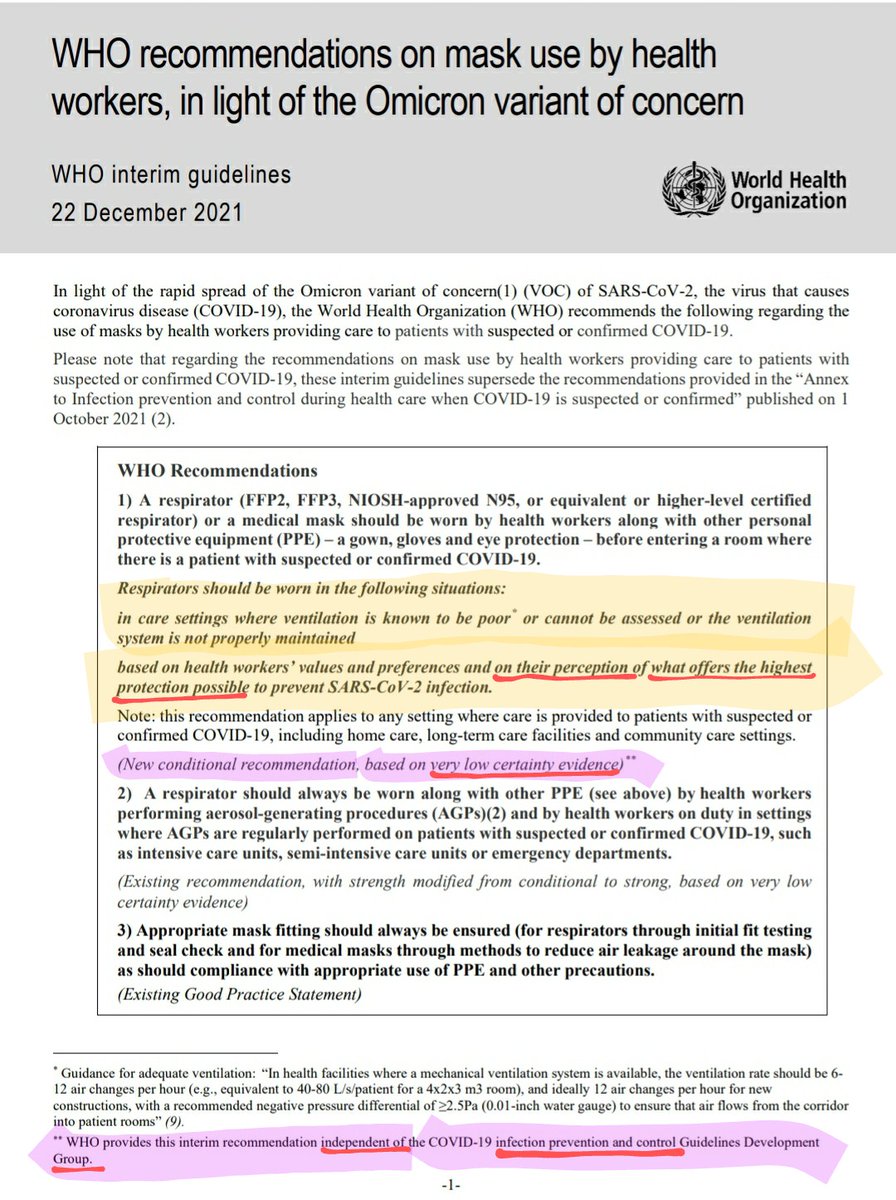
This statement is pure negligence. They have been running this unethical trial for 2 years. This is human experimentation - there is no equipoise for this study. A Respirator, designed to protect against an INHALED HAZARD, will BY DEFINITION, work better than a droplet mask.
5/
5/

They are using nurses like guinea pigs, waiting to see how many fall ill, rather than following the advice of Occupational Hygienists and other Aerosol experts, who have been loudly calling for Respiratory PPE.
These folks would RCT parachutes/gravity
6/
These folks would RCT parachutes/gravity
6/
https://twitter.com/kate_cole_/status/1384338584295989249?t=U0Ba-5cCCPrlSIC1BwRGOg&s=19
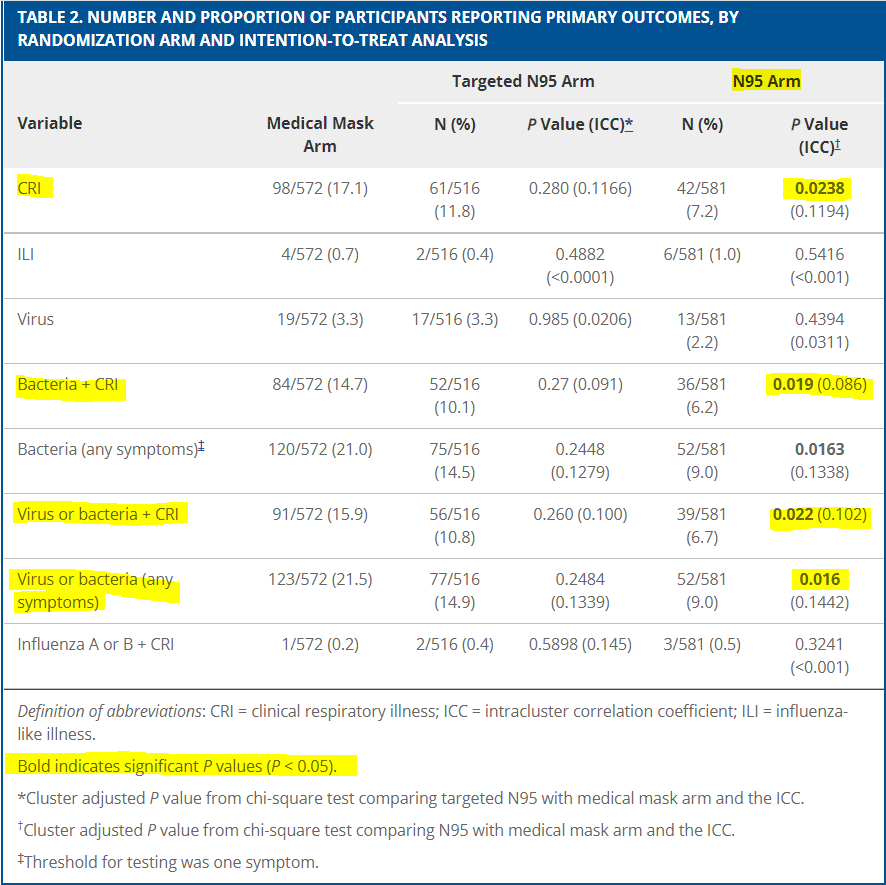
Regarding these precious RCTs... Lynora frequently references Radonovich.
That study was a joke, and was designed to fail. All it proves is that #DropletDogma doesn't work.
7/
That study was a joke, and was designed to fail. All it proves is that #DropletDogma doesn't work.
7/
https://twitter.com/CPita3/status/1451771507546509314?t=MvuWOOUhKreJ5xD6khZKZw&s=19
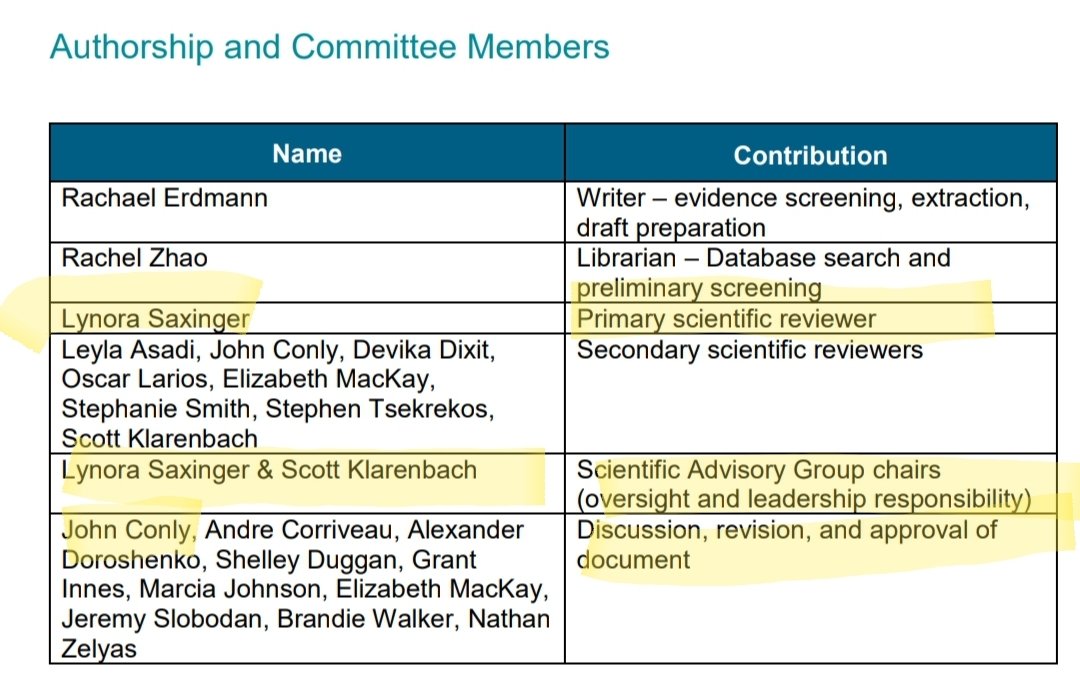
Lynora/Conly's AHS SAG also launders this misinformation via their erroneous Rapid Reviews, which reference Conly’s own problematic Systematic Review, like an ouroboros of BS.
Read this thread and do some investigative journalism please.
/end
Read this thread and do some investigative journalism please.
/end
https://twitter.com/CPita3/status/1452498957930741761?t=MvuWOOUhKreJ5xD6khZKZw&s=19
• • •
Missing some Tweet in this thread? You can try to
force a refresh