🚨 ATTENTION: Alberta Healthcare Workers, Patients:
Despite the catastrophic situation unfolding in your hospitals, and the uncontrolled spread of Delta in your communities, do not expect @AHS_media to provide HCWs with Respiratory PPE (N95s) anytime soon.
🧵1/
Despite the catastrophic situation unfolding in your hospitals, and the uncontrolled spread of Delta in your communities, do not expect @AHS_media to provide HCWs with Respiratory PPE (N95s) anytime soon.
🧵1/



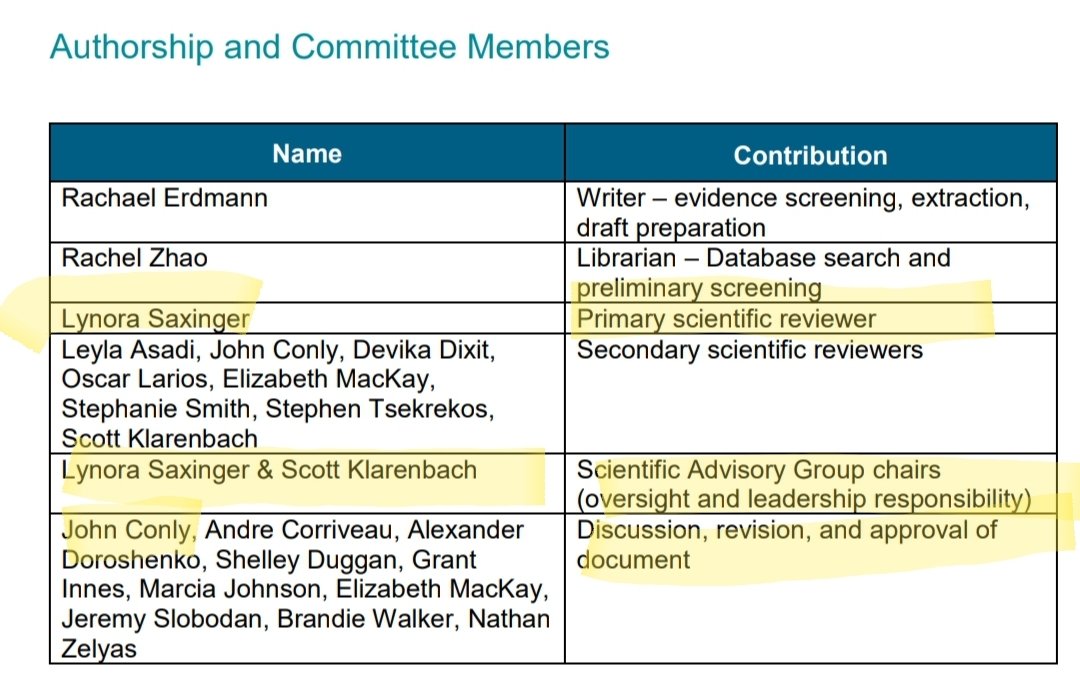
The @AHS_media SAG has just released a 73 page, biased, diatribe against the efficacy of Respiratory Protective Equipment - which can best be described as Decision-Based Evidence Making. I'm sure the AHS lawyers were pleased with this report.
2/
2/
https://twitter.com/caruzycki/status/1439313428552634368?s=19
It's no secret that Alberta IPAC requires HCWs to use surgical masks when treating COVID patients, despite overwhelming evidence that SARS2 transmits via *INHALED* aerosols.
Not a shock that the usual #DropletDogma suspects concluded this was A-OK.
3/
Not a shock that the usual #DropletDogma suspects concluded this was A-OK.
3/
https://twitter.com/jvipondmd/status/1433179787028275204?s=19
First, let's review the facts.
SARS2 is transmitted via *INHALED* Aerosols that an infectious person exhales.
Both the CDC and WHO now acknowledge this fact. The key admission is that the virus is *INHALED*. That means Respiratory PPE (N95s) are required to protect HCWs.
4/
SARS2 is transmitted via *INHALED* Aerosols that an infectious person exhales.
Both the CDC and WHO now acknowledge this fact. The key admission is that the virus is *INHALED*. That means Respiratory PPE (N95s) are required to protect HCWs.
4/




Despite the AHS SAG's attempts to muddy the waters, there is ZERO scientific doubt that SARS2 is transmitted via inhaled Aerosols.
There is evidence that the aerosol route leads to more severe disease and that the VOCs are becoming more efficient at aerosol transmission.
5/
There is evidence that the aerosol route leads to more severe disease and that the VOCs are becoming more efficient at aerosol transmission.
5/

Even the dogmatic AHS SAG knows it would be foolish to come out strongly against Aerosol transmission.
So instead, they muddy the waters (suggest it's still an open question), and then side-step the issue all together.
6/
So instead, they muddy the waters (suggest it's still an open question), and then side-step the issue all together.
6/


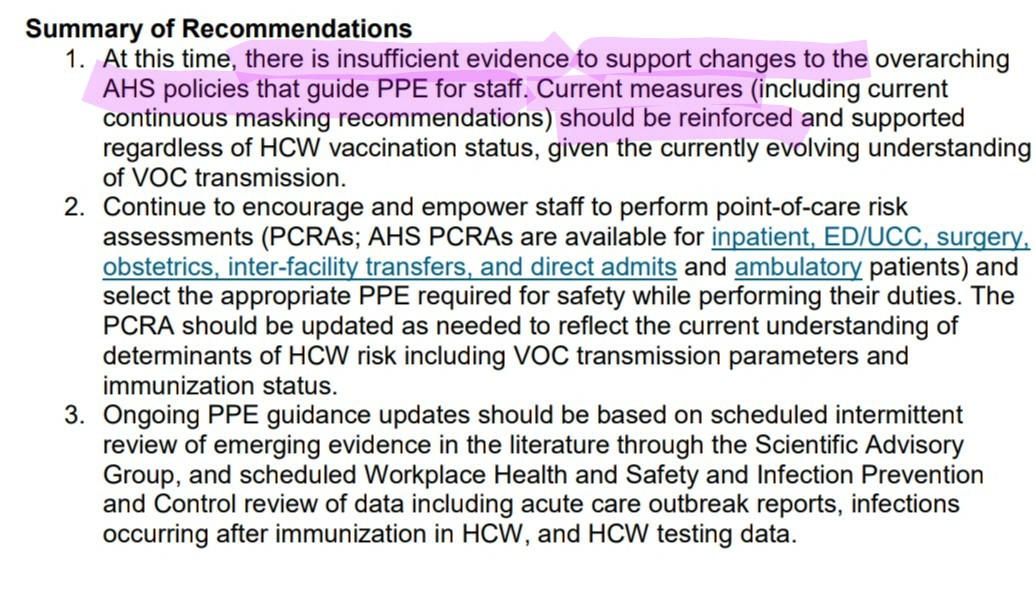
Don't bother reading all 73 pages, this is the most important statement in the document:
"It is not presumed that the possibility of aerosol transmission should alone mandate the use of respirator N95 masks"
7/
"It is not presumed that the possibility of aerosol transmission should alone mandate the use of respirator N95 masks"
7/

Think about what this means... the SAG is not denying Aerosol transmission occurs... they're saying that EVEN IF the virus transmits via inhaled aerosols... that Respiratory Protective Equipment (RPE) FUNDAMENTALLY DOES NOT WORK!
8/
8/


This is a pretty revolutionary finding - I'm surprised the media isn't covering it.
"AHS Scientific Advisory Group finds that Respiratory Protective Equipment is useless"
Their Occuaptional Health & Safety colleagues must be devastated - A life's work in ruins. Short 3M?
9/
"AHS Scientific Advisory Group finds that Respiratory Protective Equipment is useless"
Their Occuaptional Health & Safety colleagues must be devastated - A life's work in ruins. Short 3M?
9/
When can we expect the Alberta OHS Code to be updated regarding this critical finding? Better scrap the OHS RPE COP - no need for this useless measure.
Who's going to let @uaxOHS know that their RPE COP is outdated? The AHS SAG is clear - there's no evidence RPE works.
10/
Who's going to let @uaxOHS know that their RPE COP is outdated? The AHS SAG is clear - there's no evidence RPE works.
10/


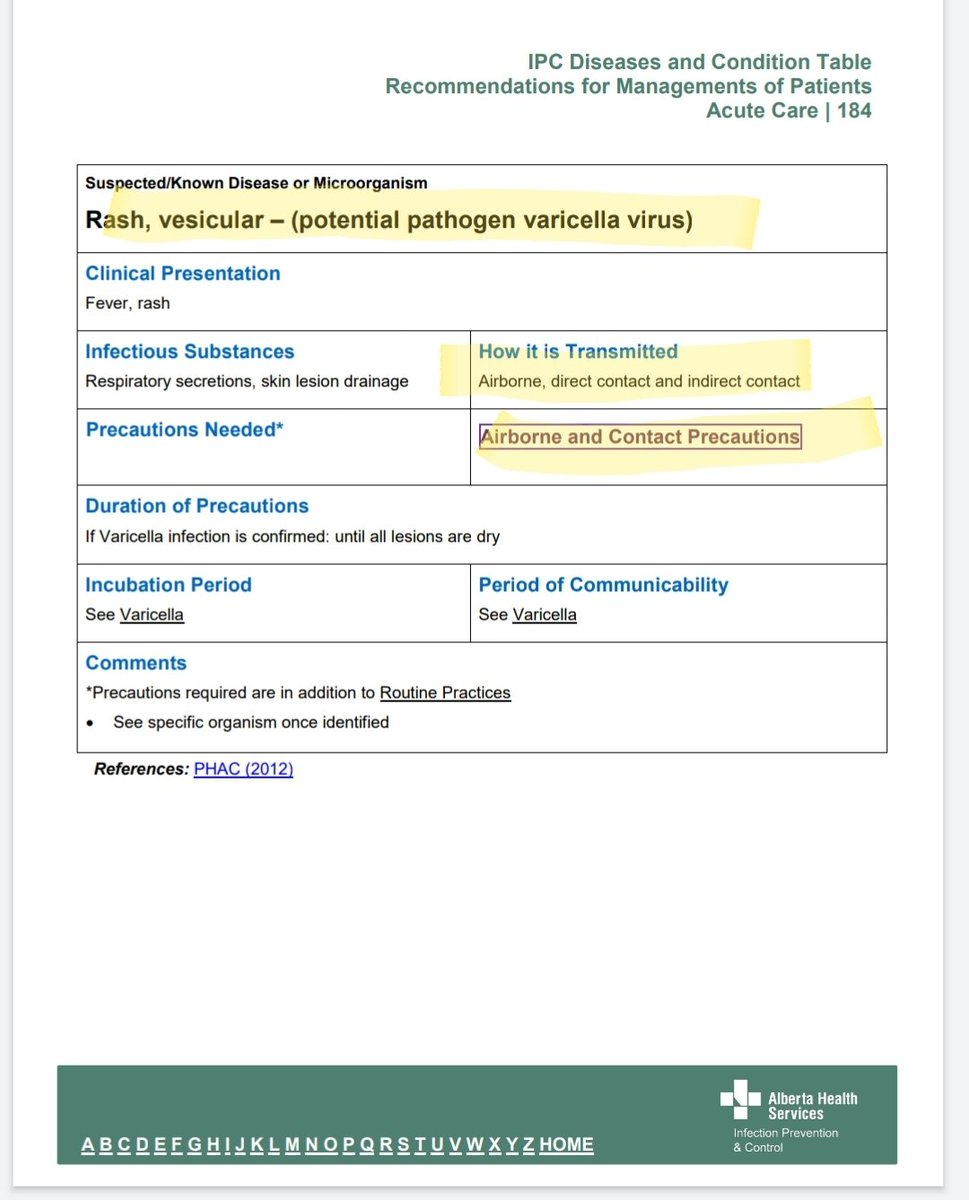
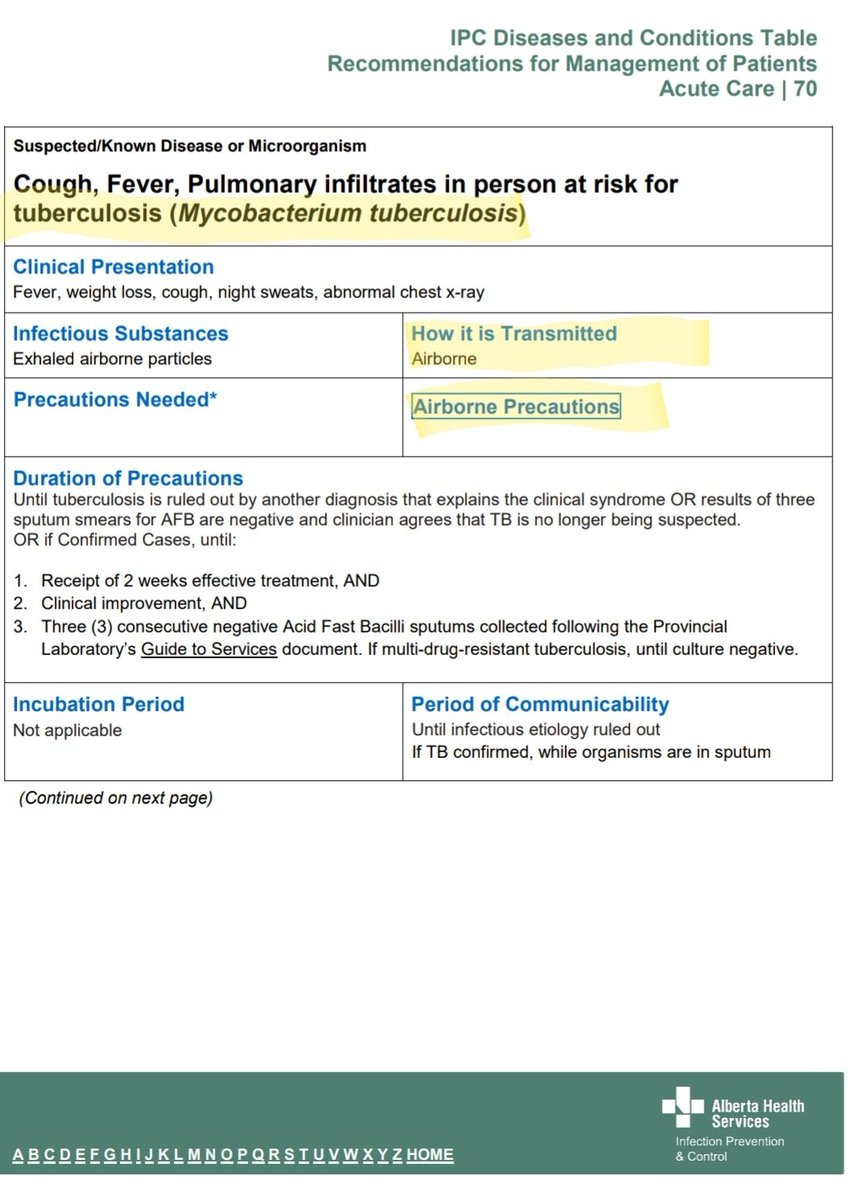
This also has implications for @AHS_media IPAC - I assume they'll be updating their Precautions guidance momentarily, to remove Airborne Precautions/Respirators from Varicella, Measles, TB and AGMPs - given the finding that N95s don't protect HCWs from aerosol inhalation.
11/
11/


So what was behind AHS SAG's groundbreaking statement, which undermines the entire OH&S RPE and IPAC fields?
They must have uncovered a pretty convincing study! I mean, it's like declaring seatbelts are harmful.. you'd need an iron clad case, right?
Let's have a look...
12/
They must have uncovered a pretty convincing study! I mean, it's like declaring seatbelts are harmful.. you'd need an iron clad case, right?
Let's have a look...
12/



So the rationale for declaring that there's no evidence N95s protect HCWs from aerosol transmission, is based on "very low to low quality evidence". The report implies we shouldn't put too much stock in it, because the evidence is "poor quality" and "very uncertain". 🤯
13/
13/



If this is true, that the body of evidence is hot garbage, and no conclusions can really be drawn from it... why isn't @AHS_media recommending HCWs upgrade to N95 respirators AS A PRECAUTION, as per the OHS standards for EVERY OTHER HAZARDOUS AEROSOL/PATHOGEN?!
14/
14/
One implication is there are unknown "harms" of N95s... think "harms of acne" argument.
This is anti-mask rubbish. Respirators are designed to be breathable. The new soft-fold respirators are extremely comfortable. Everyone I know that has upgraded, has preferred them.
15/
This is anti-mask rubbish. Respirators are designed to be breathable. The new soft-fold respirators are extremely comfortable. Everyone I know that has upgraded, has preferred them.
15/

There are 2 additional points in the report that stood out as borderline intentional misinformation, which need to be addressed:
1) No evidence variants behave differently in the environment ❌
2) No jurisdictions changed their guidance in response to transmissible VOCs ❌
16/
1) No evidence variants behave differently in the environment ❌
2) No jurisdictions changed their guidance in response to transmissible VOCs ❌
16/

Both of these statements are false - egregiously so.
Re. 1) The study by Adenaiye, Milton et al, found a significant increase in aerosol viral RNA for Alpha, and concluded that SARS2 is evolving toward more efficient aerosol generation.
17/
academic.oup.com/cid/advance-ar…
Re. 1) The study by Adenaiye, Milton et al, found a significant increase in aerosol viral RNA for Alpha, and concluded that SARS2 is evolving toward more efficient aerosol generation.
17/
academic.oup.com/cid/advance-ar…

Re. 2) The SAG attempts to cherry-pick jurisdictions that re-inforce their IPAC dogma. Notice the absence of USA and all Asian nations? (hint: they support N95s for COVID).
In addition, Australia DID update their national guidance for N95s BECAUSE of transmissible VOCs!
18/
In addition, Australia DID update their national guidance for N95s BECAUSE of transmissible VOCs!
18/




In case this thread looks familiar, it's because the AHS SAG has pulled a similar stunt with respect to HEPA filtration. This group is opposed to ALL physics-based precautionary measures to mitigate Airborne transmission.
19/
19/
https://twitter.com/CPita3/status/1416793141781348354?s=19
How much tax payer money was spent generating this 73 page document, which will be used to deny N95s to HCWs during a catastrophic surge, where hospitals are overwhelmed?
And how is the status-quo #DropletDogma working out in Alberta hospitals?
Not well.
20/
And how is the status-quo #DropletDogma working out in Alberta hospitals?
Not well.
20/




Here's how well #DropletDogma and the PCRA process is working out in Ontario:
21/
thestar.com/news/gta/2021/…
21/
thestar.com/news/gta/2021/…
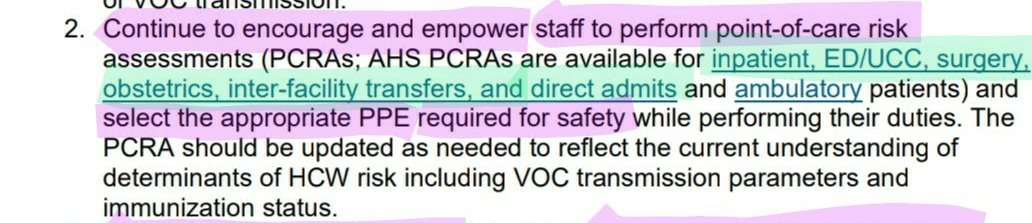
Don't let anyone gaslight you and say, "but HCWs have access to respirators through the PCRA!". That loophole isn't working; HCWs are brainwashed/pressured into using surgical masks. And patients don't get a say.
Here's the linked PCRA... can anyone spot the word N95?
22/
Here's the linked PCRA... can anyone spot the word N95?
22/

This isn't just an Alberta problem... Ontario IPAC MDs are just as intransigient:
23/
23/
https://twitter.com/CPita3/status/1435054063561756676?s=19
This is an international failing of the IPAC field. For those in IPAC, that care about the credibility and respect of your field going forward, now is the time to speak out.
24/
24/
https://twitter.com/CPita3/status/1428566078007959558?s=19
.@AHSMedia, for the sake of Alberta HCWs and patients, who are facing an unfathomable crisis - #ReleaseTheN95s.
Enough BS - we need to throw every tool in the toolbox at the virus right now.
It is negligent and inconceivable that you continue to keep the RPE locked up.
/end
Enough BS - we need to throw every tool in the toolbox at the virus right now.
It is negligent and inconceivable that you continue to keep the RPE locked up.
/end
PS.
If anyone wants to read a proper ID/IPAC analysis of this issue, please read this by Dr. Klompas (all of his work was notably absent from the SAG review):
academic.oup.com/cid/advance-ar…
If anyone wants to read a proper ID/IPAC analysis of this issue, please read this by Dr. Klompas (all of his work was notably absent from the SAG review):
academic.oup.com/cid/advance-ar…
• • •
Missing some Tweet in this thread? You can try to
force a refresh