
Hey 👋 #MedStudentTwitter. Fancy for some quick ABG practice you’ll see commonly in the MICU? 😊🧵#MedEd #MedTwitter
80F with unknown history presents to ED after being found down 😵. ABG admission:
1/
80F with unknown history presents to ED after being found down 😵. ABG admission:
1/

Before we start, do you remember your normal ABG values? It’s easy. Just remember the “rule of 4 🍀”
pH: 7.40
pCO2: 40
HCO3: 24
2/
pH: 7.40
pCO2: 40
HCO3: 24
2/
First look at pH
↓pH 7.19 = acidemia
Next determine if primary problem is metabolic (HCO3🧪) or respiratory (CO2😮💨)
↑↑pCO2 105 & ↑↑HCO3 39
What here would give us an acidosis? The high pCO2
So this is a 1° respiratory acidosis
3/
↓pH 7.19 = acidemia
Next determine if primary problem is metabolic (HCO3🧪) or respiratory (CO2😮💨)
↑↑pCO2 105 & ↑↑HCO3 39
What here would give us an acidosis? The high pCO2
So this is a 1° respiratory acidosis
3/
Now 👀 at compensation
If ↑pCO2😮💨resp acidosis
What should kidneys do?
↑HCO3🧪metabolic alkalosis
pCO2 &HCO3 in SAME direction=compensation
✔️pH to 👀 if compensated
If pH
➤normal=compensated✔️
➤very abnormal=uncomp❌❌
➤tad abnormal=partial comp❌
scientific I kno 😂
4/
If ↑pCO2😮💨resp acidosis
What should kidneys do?
↑HCO3🧪metabolic alkalosis
pCO2 &HCO3 in SAME direction=compensation
✔️pH to 👀 if compensated
If pH
➤normal=compensated✔️
➤very abnormal=uncomp❌❌
➤tad abnormal=partial comp❌
scientific I kno 😂
4/
Let’s summarize our case:
↑↑pCO2 105
↑ HCO3 39
↓ pH 7.19
↑↑pCO2 = we said 1° respiratory acidosis 😮💨
↑ HCO3 = kidneys compensating via metabolic alkalosis 🧪
↓ pH = kidneys not compensating enough 😪
✅ Uncompensated acute on chronic respiratory acidosis
5/
↑↑pCO2 105
↑ HCO3 39
↓ pH 7.19
↑↑pCO2 = we said 1° respiratory acidosis 😮💨
↑ HCO3 = kidneys compensating via metabolic alkalosis 🧪
↓ pH = kidneys not compensating enough 😪
✅ Uncompensated acute on chronic respiratory acidosis
5/
The math isn’t necessary, but for fun
Expected 🧪metabolic compensation for 😮💨🫁 acidosis:
ACUTE: “10 for 1”
- Each 10 pCO2>40, HCO3 ↑1
CHRONIC “10 for 4”
- Each 10 pCO2>40, HCO ↑4
pCO2 105
HCO3 39
If acute, expect HCO3 ↑6
If chronic, expect HCO3 ↑24
Actual HCO3 ↑15
6/
Expected 🧪metabolic compensation for 😮💨🫁 acidosis:
ACUTE: “10 for 1”
- Each 10 pCO2>40, HCO3 ↑1
CHRONIC “10 for 4”
- Each 10 pCO2>40, HCO ↑4
pCO2 105
HCO3 39
If acute, expect HCO3 ↑6
If chronic, expect HCO3 ↑24
Actual HCO3 ↑15
6/
Also, it’s good practice to always calculate anion gap even if they don’t have a metabolic acidosis
Na - (HCO3+Cl)
but was normal, so let’s ignore🙃
7/
Na - (HCO3+Cl)
but was normal, so let’s ignore🙃
7/
Ah yes, your classic CO2 retainer (ie COPD 🫁)
acutely decompensating (think COPD exacerbation🦠, drugs💊, stroke🧠, etc)
Baseline: chronic resp acidosis ↑pCO2 + compensatory ↑HCO3 = normal pH
Acutely: worse resp acidosis ↑↑pCO2 and kidneys not fully compensated (↓pH)
8/
acutely decompensating (think COPD exacerbation🦠, drugs💊, stroke🧠, etc)
Baseline: chronic resp acidosis ↑pCO2 + compensatory ↑HCO3 = normal pH
Acutely: worse resp acidosis ↑↑pCO2 and kidneys not fully compensated (↓pH)
8/
Learners you will soon recognize this common patter of acute on chronic resp acidosis 🙃
-Hella high pCO2 (but not dead 😮)
-Hella high HCO3 (but pH still low)
-Though pH not as low as you’d expect with that pCO2
So this pt comes into your ED altered .…what ru gonna do 🩺?
9/
-Hella high pCO2 (but not dead 😮)
-Hella high HCO3 (but pH still low)
-Though pH not as low as you’d expect with that pCO2
So this pt comes into your ED altered .…what ru gonna do 🩺?
9/
The problem is ventilation, not oxygenation. We need to blow off CO2. Eliminate C/D.
NIPPV (BiPAP) might be ok if pt was alert/cooperative
But our pt is obtunded, can’t protect airway
Intubate! (while eval/treating underlying cause)
10/
NIPPV (BiPAP) might be ok if pt was alert/cooperative
But our pt is obtunded, can’t protect airway
Intubate! (while eval/treating underlying cause)
10/
What vent settings could you adjust to fix her respiratory acidosis?
11/
11/
↑RR (or ↑tidal volume. Usually Tv is set based on ideal body weight)
I like this simple infographic by CORE IM
12/
I like this simple infographic by CORE IM
12/
https://twitter.com/coreimpodcast/status/1248946878378586113
Patient’s mental status quickly improved on the vent
However the next morning she fails her SBT (spontaneous breathing trial) for the following reason:
“RR<4. Awake & nodding head, but would not breathe”
You get a repeat ABG (left) & immediately know why she’s apneic! 🤨
13/
However the next morning she fails her SBT (spontaneous breathing trial) for the following reason:
“RR<4. Awake & nodding head, but would not breathe”
You get a repeat ABG (left) & immediately know why she’s apneic! 🤨
13/

Under normal conditions, what is the main determinant of respiratory drive?
While of the above affect resp drive, normally pCO2 is the main regulator
Central chemoreceptors in the medulla🧠 respond to pH of CSF
pCO2 (lipid soluble) easily crosses BBB to affect CSF pH
So
↓pCO2 (hypocapnia)
↑pH CSF
↓central chemoreceptor stim
↓RR -► apnea
15/
Central chemoreceptors in the medulla🧠 respond to pH of CSF
pCO2 (lipid soluble) easily crosses BBB to affect CSF pH
So
↓pCO2 (hypocapnia)
↑pH CSF
↓central chemoreceptor stim
↓RR -► apnea
15/
Apneic threshold: pCO2 below which central resp drive stops
We’ve overventilated our pt😮💨, ↓pCO2, & she no longer has sufficient pCO2 to drive spontaneous resp
But her pCO2 is normal? Recall she normally lives at higher pCO2. This is ↓ for her. We know this by her ↑pH
16/
We’ve overventilated our pt😮💨, ↓pCO2, & she no longer has sufficient pCO2 to drive spontaneous resp
But her pCO2 is normal? Recall she normally lives at higher pCO2. This is ↓ for her. We know this by her ↑pH
16/

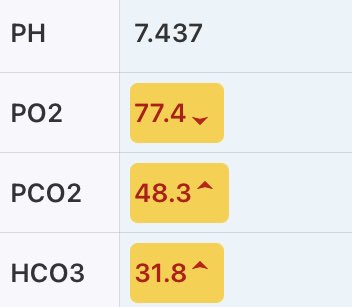
Vent settings are adjusted to reduce the RR
Repeat ABG in the PM is drawn as below (closer to her baseline). She passes her SBT & is successful extubated 😁
Ez clap 👏🏼. Lmk if this helps you on your ICU wards & if you have any other thoughts!
17/
Repeat ABG in the PM is drawn as below (closer to her baseline). She passes her SBT & is successful extubated 😁
Ez clap 👏🏼. Lmk if this helps you on your ICU wards & if you have any other thoughts!
17/
To clarify:
For HCO3, I usually use from
- BMP (HCO3 measured in blood)
- vs. ABG (HCO3 calculated from the pH/pCO2)
- but in most cases (like here) they are similar, so I just used single ABG for simplicity
& I forgot to attach last ABG :)
18/
For HCO3, I usually use from
- BMP (HCO3 measured in blood)
- vs. ABG (HCO3 calculated from the pH/pCO2)
- but in most cases (like here) they are similar, so I just used single ABG for simplicity
& I forgot to attach last ABG :)
18/
• • •
Missing some Tweet in this thread? You can try to
force a refresh


