
There have been a number of recent studies that haven't really reached MSM - highlighting the complex biology of long COVID. TL;DR: Long COVID & even 'mild' infection is associated with:
- long term immune dysregulation and inflammation
- virus persistence
- neuro-inflammation
- long term immune dysregulation and inflammation
- virus persistence
- neuro-inflammation
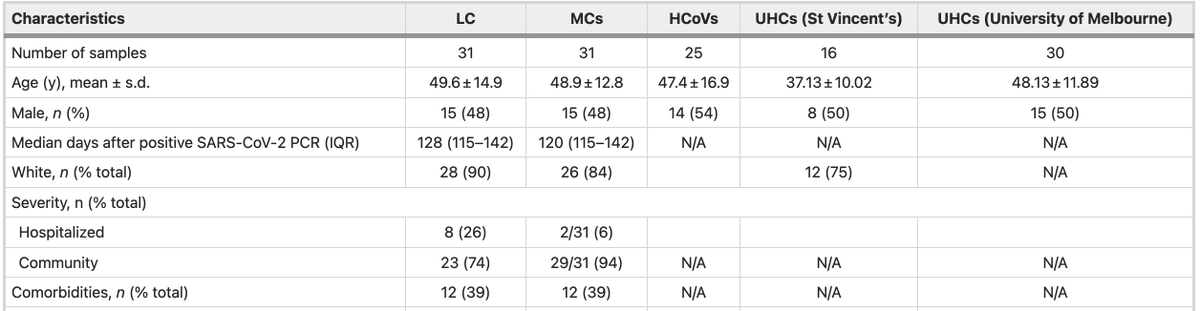
Here's a study of 147 people with SARS-CoV-2 infection - of whom 31 had long COVID (fatigue, breathlessness or chest pain at 4 months). These patients were compared with 31 age, & gender matched controls who had symptomatic acute illness but no long COVID.
nature.com/articles/s4159…
nature.com/articles/s4159…
They were also compared to uninfected healthy donors (UHDs) who were essentially healthy patients who had provided research samples before 2019, as well as patients who had been infected with other seasonal coronaviruses (not SARS-CoV-2). Levels of 28 biomarkers were compared.
Characteristics of patients were very similar, and the vast majority of both cases and controls had 'mild' acute infection, although a higher proportion of those who went onto develop long COVID had been hospitalised compared to those who didn't (26% vs 6%) 
Patients had repeated measurements of markers done from blood up to 8 months. While there was no difference in biomarkers at 4 months post-infection between those who developed long COVID & those who didn't - both gps had higher levels of markers than those without infection.
But both long COVID cases & controls (no long COVID post-infection) had higher levels of 6 biomarkers than uninfected controls (pre-pandemic healthy controls, or those infected by other human coronaviruses). IFN-β was 7-8x ⬆️ in those infected at 4 months compared to uninfected.
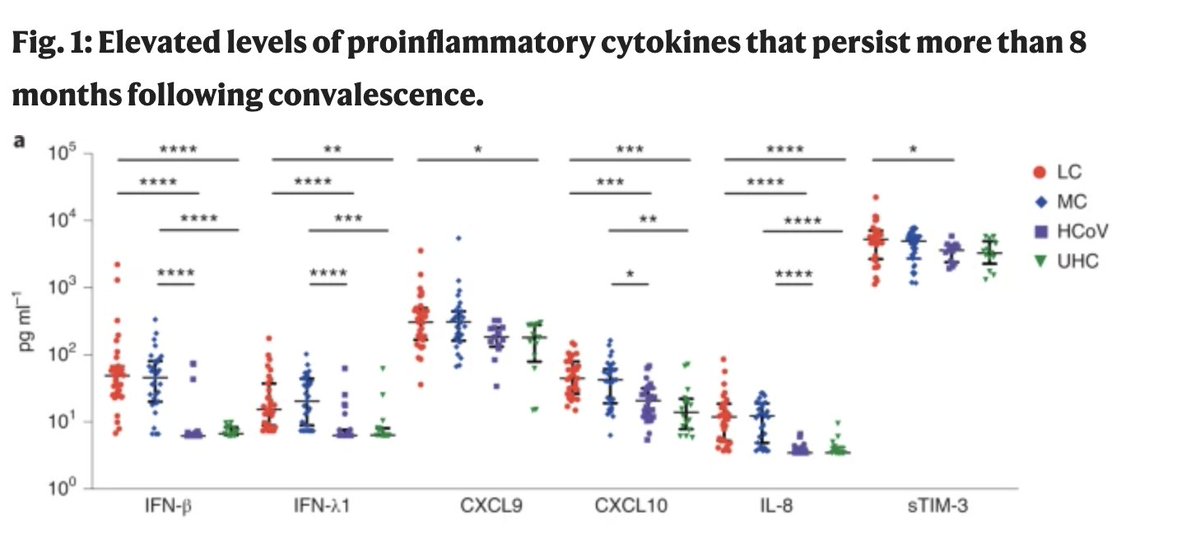
While many of these reduced at the 8 month time point for the non-long COVID control group (MC), they *remained high* for the long COVID group. IFN-β & IFN-λ1 remained elevated in the long COVID group compared to the non-long COVID infected group, & uninfected controls.
The elevation of biomarkers was so consistent that the authors were able to build a prediction model for long COVID based on the markers in their blood at *8 months* which predicted them as having long COVID with 80% accuracy simply from the levels of markers in their blood.
The authors then compared the immune cell response and types of immune cells in people with long COVID compared with those who did not have long COVID post-infection. They found substantial differences.
There was chronic activation of a type of CD8+ T cells, that are important for virus clearance. As well as signs of T cell exhaustion, and absence of naive T and B cell subsets - all of which suggest long-term impact on the immune system.
What this means in practical terms is unclear- but concerning nevertheless. There are several ways immune dysregulation can mainfest - immune deficiency against other pathogens, auto-immune disease, or even cancer (several viruses have been linked with cancer yrs later).
Understanding what this immune dysregulation that was clearly present at least at 8 months, and possibly longer means will take time, but this shows that long COVID clearly shows a different immunological profile compared to people who don't have persistent symptoms.
Whether this is because of persistence of virus, or virus antigen, or auto-immunity post-infection isn't known yet. It could be one of these, or even a combination - but all possibilities should concern us.
Another preprint from @VirusesImmunity & others, that came out recently with rather concerning findings. They studied the brains of humans and mice with 'mild' SARS-CoV-2 infection. Autopsies were done 9 people who died of other causes while infected or few wks post-infection.
Compared to autopsies in 5 people without infection, brain tissue showed microglial reactivity in subcortical white matter. Microglia are an immune cell found in the brain, and microglial reactivity is often associated with neurodegeneration.
biorxiv.org/content/10.110…
biorxiv.org/content/10.110…
Microglial reactivity can impair the generation of new neurons in the hippocampus, the part of the brain responsible for memory formation. The investigators found similar findings in the mouse brain as well
Mice brains also showed increased microglial reactivity - in hippocampal white matter at 7-days post-infection persisting until at least 7-weeks post-infection. Generation of new neurons in the hippocampus was also reduced in mice.
The scientists also compared people with long COVID and 'brain fog' with those with long COVID without cognitive symptoms. They found elevated inflammatory markers (CCL11 cytokine levels) in the blood of people
suffering from long-COVID with and without brain fog
suffering from long-COVID with and without brain fog
Another recent study examined autopsies from people who had been infected with SARS-CoV-2 up to 230 days ago- including some who had mild/asymptomatic infection (died from other causes) - showing long-term persistence of virus in multiple tissues.
assets.researchsquare.com/files/rs-11390…
assets.researchsquare.com/files/rs-11390…
*All* 44 people autopsied had virus RNA in at least one tissue- 98% in the lung; heart (80%); lymphoid tissue (86%), gut (73%), kidney/endocrine tissue (64%); reproductive (42.5%); muscle, skin, adipose, and peripheral nervous tissue (68.2%); eye (58%), brain (91%)
The authors also looked at sub-genomic virus RNA (sgRNA) and cell culture to examine whether virus in these tissues was dead or was likely to be replicating. sgRNA was detected in multiple tissues even after a month in 43% of the autopsies & even at day 99 in a late autopsy.
This suggests dissemination of SARS-CoV-2 to multiple tissues and virus persistence for long periods of time- up to 230 days in heart, lung, brain and eye. Multi-system involvment seems to occur even in those with mild infection, as seen in the autopsy of a child in this series.
Previous work has also shown long-term persistence of the virus in olfactory neuro-epithelium of those who have loss of smell post COVID-19 - with persistence up to 6 months
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
All these studies clearly show immunological & inflammatory correlates of long COVID and neuro-inflammation in brains of people with long COVID. This appears to occur even in those with mild infection. We also see virus persistence in multiple organs for long durations.
I'd really like to see those suggesting long COVID is 'psychosomatic' or not something to be concerned about explain how we can actually predict long COVID with reasonable accuracy simply from looking at blood markers of people post-infection.
We know that many viruses have been associated with severe complications- inflammatory, auto-immune and cancers- decades later. Very recent paper on association between EBV and multiple sclerosis.
science.org/doi/10.1126/sc…
science.org/doi/10.1126/sc…
It's going to take years to understand the full impact on SARS-CoV-2, but the fact that it's causing long-term illnesses far more common that we've seen with many other viruses, including neuro-cognitive dysfunction is very worrying.
The symptoms appear to correlate with inflammatory biomarkers, and long-term immune dysregulation which could be related to viral persistence. We really need to stop treating this as an acute illness alone, and one where infection is benign. It's not.
Anyone reading the extensive literature now on the long term impacts of the virus on multiple organ systems, and the immune system would be very worried about what the future holds. We've had millions of people infected in single weeks at points. What will this mean for them?
I know the acute toll of COVID-19 has been terrible, but if we continue to ignore the long-term toll, we are risking the health of millions of people across the globe with a virus we know persists in multiple tissues, and is associated with multiple markers of neuro-degeneration.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



