
#JanuAIRWAY Day 24 -Paediatric Airways. (ft. expert contributions from Alistair Baxter and @ENT_UK’s Adam Donne). Let’s dive in … Here's some #OnePagers covering anatomy, induction, airway manoeuvres and basic airway equipment.
#JanuAIRWAY 1/10
#JanuAIRWAY 1/10




Top tip from Alistair Baxter: Remember that a Macintosh blade is a hyperangulated blade in an infant and requires an intubation stylet shaped to match the curve of the blade
#JanuAIRWAY 2/10
#JanuAIRWAY 2/10
The difficult paediatric airway = #SCARY. Upper airway obstruction in children – broad range of presentations, three important diagnoses; Croup, Epiglottitis and Inhaled Foreign Body. Here’s some #OnePagers.
#JanuAIRWAY 3/10
#JanuAIRWAY 3/10


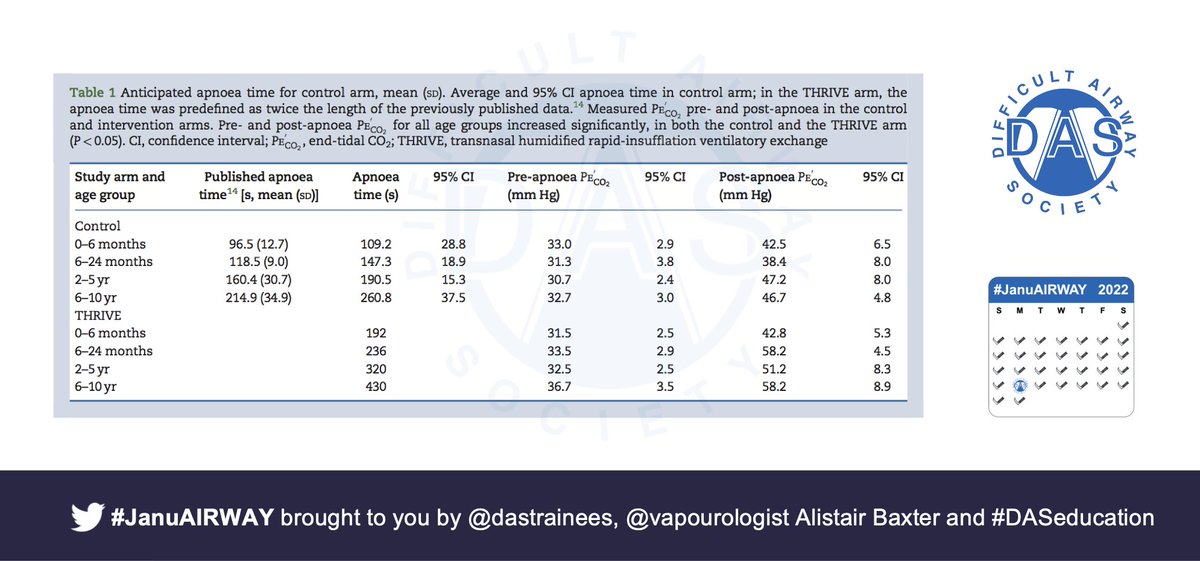
TIVA is ever increasing in popularity as is “O”s up the nose. HFNO is generally well tolerated, can add peep with a pacifier and allows a true tubeless field. Here’s a #OnePager
🔗pubmed.ncbi.nlm.nih.gov/28100527/
🔗onlinelibrary.wiley.com/doi/abs/10.111…
#JanuAIRWAY 4/10
🔗pubmed.ncbi.nlm.nih.gov/28100527/
🔗onlinelibrary.wiley.com/doi/abs/10.111…
#JanuAIRWAY 4/10

Good laryngoscopy technique in children is important to prevent airway trauma. VL can be useful in children but evidence is mixed.
🔗ncbi.nlm.nih.gov/books/NBK24811…
🔗journals.lww.com/ejanaesthesiol…
🔗pubmed.ncbi.nlm.nih.gov/26705976/
🔗pubmed.ncbi.nlm.nih.gov/34103817/
#JanuAIRWAY 5/10
🔗ncbi.nlm.nih.gov/books/NBK24811…
🔗journals.lww.com/ejanaesthesiol…
🔗pubmed.ncbi.nlm.nih.gov/26705976/
🔗pubmed.ncbi.nlm.nih.gov/34103817/
#JanuAIRWAY 5/10

Why not review the #One pagers from Day 7 on laryngoscopy, the position theory and different device DL and VL devices?
🔗
#JanuAIRWAY 6/10
🔗
https://twitter.com/dastrainees/status/1479360148590239746?s=20
#JanuAIRWAY 6/10
Most VL devices have paediatric blades available. Question #MedTwitter do you have paediatric VL available in your department?
#JanuAIRWAY 7/10
#JanuAIRWAY 7/10
Fibreoptic intubation is an advanced technique that requires attention to detail and management of multiple different aspects. Intubation via a SAD is a nice technique. Here’s a #OnePager covering the essentials.
#JanuAIRWAY 8/10
#JanuAIRWAY 8/10

Here are some papers / links that you might find interesting:
🔗rch.org.au/clinicalguide/…
🔗pubmed.ncbi.nlm.nih.gov/20816545/
🔗das.uk.com/guidelines/pae…
🔗bjanaesthesia.org.uk/article/S0007-…
🔗academic.oup.com/bja/article/11…
🔗sjtrem.biomedcentral.com/articles/10.11…
🔗bjanaesthesia.org.uk/article/S0007-…
#JanuAIRWAY 9/10
🔗rch.org.au/clinicalguide/…
🔗pubmed.ncbi.nlm.nih.gov/20816545/
🔗das.uk.com/guidelines/pae…
🔗bjanaesthesia.org.uk/article/S0007-…
🔗academic.oup.com/bja/article/11…
🔗sjtrem.biomedcentral.com/articles/10.11…
🔗bjanaesthesia.org.uk/article/S0007-…
#JanuAIRWAY 9/10
Hope that helps. Tomorrow we’ll look at the obstetric airway (ft. expert contributions from @noolslucas). See you then! #JanuAIRWAY 10/10
*Disclaimer: Inclusion of content (equipment, techniques and scoring systems etc.) in #JanuAIRWAY does not constitute DAS endorsement
*Disclaimer: Inclusion of content (equipment, techniques and scoring systems etc.) in #JanuAIRWAY does not constitute DAS endorsement
• • •
Missing some Tweet in this thread? You can try to
force a refresh



















