What happens
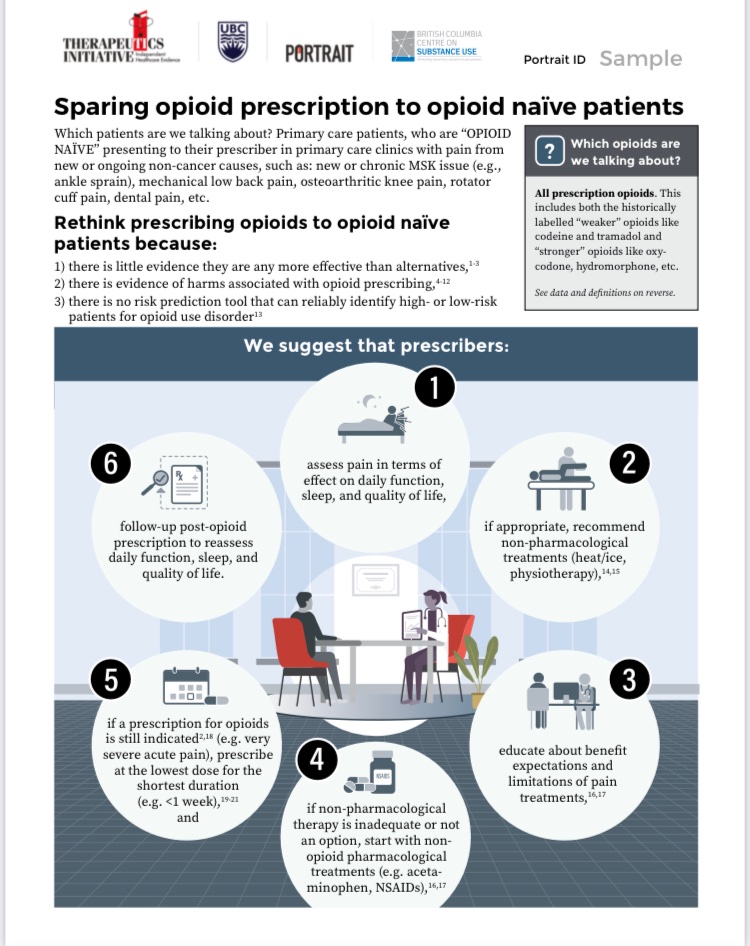
when your
family doctor
orders
LAB TESTS
for you?
Another 🧵 about the inner workings of 🇨🇦 primary care (or how the sausage gets made), and how fixing the #familydoctorshortage is not just about hiring more doctors.
@BCFamilyDoctors
when your
family doctor
orders
LAB TESTS
for you?
Another 🧵 about the inner workings of 🇨🇦 primary care (or how the sausage gets made), and how fixing the #familydoctorshortage is not just about hiring more doctors.
@BCFamilyDoctors
Let's say you go to your doctor,
after considering your story (= reason for your visit), your past medical history,
the possible diagnoses/treatments
for the issue,
she decides to order blood work (=evidence-based medicine),
& you agree with that (=shared decision making).
after considering your story (= reason for your visit), your past medical history,
the possible diagnoses/treatments
for the issue,
she decides to order blood work (=evidence-based medicine),
& you agree with that (=shared decision making).
She creates a LAB REQUISITION (="req")
She selects the tests that she thinks will help understand/treat/monitor the issue.
This is based on what she learned in med school, what she learned staying up to date(=Continuing Medical Education) & sometimes, a specialist's advice
She selects the tests that she thinks will help understand/treat/monitor the issue.
This is based on what she learned in med school, what she learned staying up to date(=Continuing Medical Education) & sometimes, a specialist's advice
She gives you the requisition, or
in COVID times,
emails it to you or
the
faxes it to the central lab intake.
You then go get the lab tests.
You need to find a lab, maybe make reappointment, maybe psych yourself up for needles.
in COVID times,
emails it to you or
the
faxes it to the central lab intake.
You then go get the lab tests.
You need to find a lab, maybe make reappointment, maybe psych yourself up for needles.
The results come back to the doctor,
via her EMR (electronic medical record),
via a third part company (in BC = @Excelleris )
The results ...
trickle back...
Let me explain this a bit more, bc the workload from this is... significant.
via her EMR (electronic medical record),
via a third part company (in BC = @Excelleris )
The results ...
trickle back...
Let me explain this a bit more, bc the workload from this is... significant.
One lab req = many EMR reports
A few years ago,
something happened in BC &
one lab req went from one set of results
to 3 to 7 sets of results.
Each one needs to be reviewed by the doctor in a timely fashion.
A few years ago,
something happened in BC &
one lab req went from one set of results
to 3 to 7 sets of results.
Each one needs to be reviewed by the doctor in a timely fashion.
every day of the week,
including weekends,
doctors need to log into the EMR,
and check and see if new results are there
In #BCPrimaryCare, many doctors do this on VACATION, because of how much work it is, and how hard it is to find vacation coverage (=locum)
including weekends,
doctors need to log into the EMR,
and check and see if new results are there
In #BCPrimaryCare, many doctors do this on VACATION, because of how much work it is, and how hard it is to find vacation coverage (=locum)
At some clinics, fellow doctors/NP's help with lab reviews.
reviewing labs ALMOST ALWAYS happens outside of clinic hours, and is part of the work not included in how primary care is currently structured.
There is no extra payment for reviewing labs, only the ~32$/visit.
reviewing labs ALMOST ALWAYS happens outside of clinic hours, and is part of the work not included in how primary care is currently structured.
There is no extra payment for reviewing labs, only the ~32$/visit.
Reviewing labs, in a timely fashion, is medicolegally required. And response to severely abnormal labs (="critical" results) needs to happen ASAP.
Obviously, if you need lab tests (based on your doctor's evidence-based assessment and your shared decision), then you should get them.
Equally obviously,
the work needed to review them
should be streamlined (stop the 7 versions!)
and
COUNTED AS PART OF THE ACTUAL WORK.
Equally obviously,
the work needed to review them
should be streamlined (stop the 7 versions!)
and
COUNTED AS PART OF THE ACTUAL WORK.
Primary care needs an organizing structure (=mesostructure), that can help describe problems like:
✖️the increase in # of reports for lab results,
✖️doctors checking labs on vacation
So that we can keep doctors doing the doctoring & minimize their admin tasks.
/Fin
✖️the increase in # of reports for lab results,
✖️doctors checking labs on vacation
So that we can keep doctors doing the doctoring & minimize their admin tasks.
/Fin
• • •
Missing some Tweet in this thread? You can try to
force a refresh