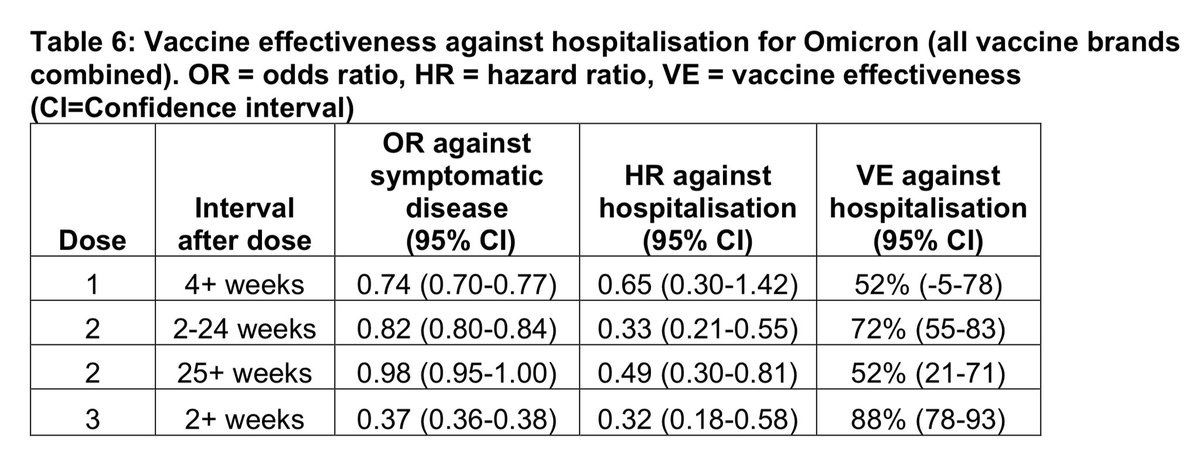
I suspect a single-dose booster won’t be enough against the omicron strain, because it’s changed so much it’s almost like a new virus. One dose wasn’t enough against the original strain, either. Two doses seems more realistic.
https://twitter.com/EricTopol/status/1489675533461831681
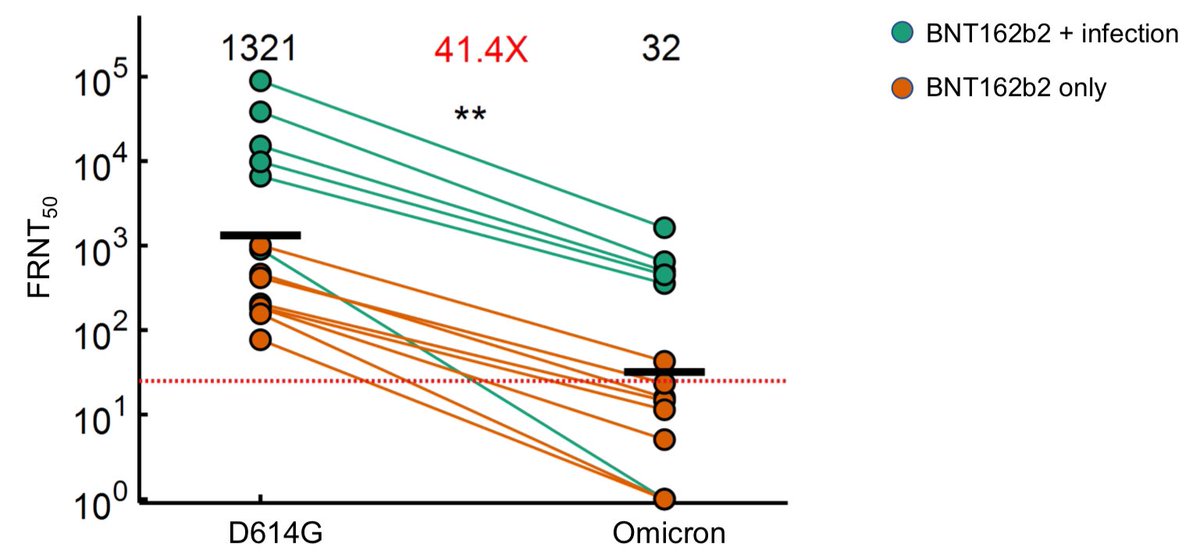
Our best bet for bringing the pandemic to a end may be nasal spray vaccines.
Early experiments suggest these may be more resistant to variants and do a much better job of preventing infection and blocking transmission than the current generation of vaccines.
Early experiments suggest these may be more resistant to variants and do a much better job of preventing infection and blocking transmission than the current generation of vaccines.
https://twitter.com/VirusesImmunity/status/1486510697332842498
But vaccines alone aren’t going to end the pandemic.
Vaccination is extremely important but we also need to make some changes to the way we live our lives. Hopefully many of these changes can be unobtrusive, such as improving ventilation & using HEPA technology to clean the air.
Vaccination is extremely important but we also need to make some changes to the way we live our lives. Hopefully many of these changes can be unobtrusive, such as improving ventilation & using HEPA technology to clean the air.
SARS-CoV-2 is one of the most transmissible viruses known to man. It doesn’t behave like flu.
It’s not seasonal, and the speed at which it moves around the globe means that we can’t predict how to update the vaccines each year in advance in the same way that we do for flu shots.
It’s not seasonal, and the speed at which it moves around the globe means that we can’t predict how to update the vaccines each year in advance in the same way that we do for flu shots.
That’s why we need to slow transmission down with a ventilation and #VaccinesPLUS strategy. This will enable us to use the vaccines that we have more effectively, leading to fewer restrictions in the long run, healthier populations, and stronger economies.
bmj.com/content/376/bm…
bmj.com/content/376/bm…
• • •
Missing some Tweet in this thread? You can try to
force a refresh