
Why yes, selective-article grabber, I did thoroughly read the BBC news article about children and NHS referrals, and I have a few comments.
#schoolclosures #UKPolitics #ENGLAND
/1
#schoolclosures #UKPolitics #ENGLAND
/1

First, it's important to note that I did what any normal human and not a data robot does when they read an infographic, I faithfully transcribed it using machine-reading software to translate it into Excel. If anyone can find the raw data, thanks.
/2
/2

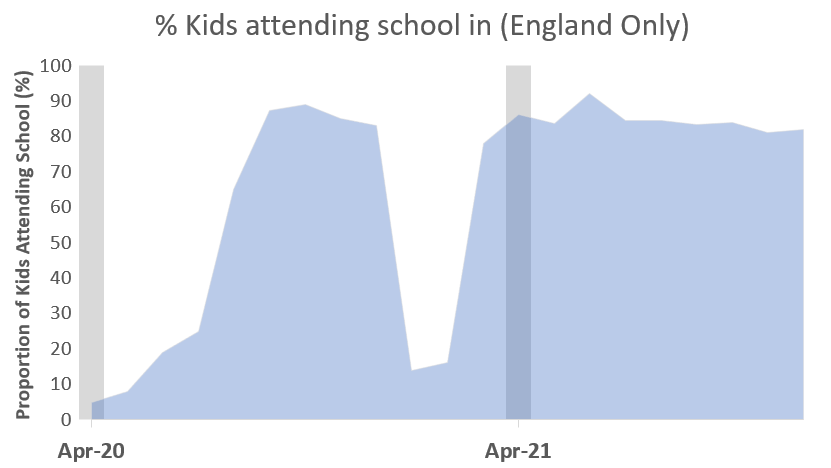
I then sourced school closures directly from gov.uk
This allowed me to create two lockdown periods (<30% school attendance) and open school periods (>75% attendance)
/3
This allowed me to create two lockdown periods (<30% school attendance) and open school periods (>75% attendance)
/3
So then I can now plot the prepandemic trend (black), and the lockdown months (red), and the school open months (blue). Visually, it appears that the first lockdown unsurprisingly led to less referrals, and then after that there was a rise.
/4
/4

Then, I created a seasonality model to create an expected model for the increasing trend while minimizing seasonal variance.
/5
/5

Now, I can estimate the variance for seasonality AND trend, and arrive to the following:
Deviance from PREPANDEMIC trend:
First closure: -27%
First opening: +27% (+54% change)
Second closure: +20% (-7% change)
Second opening: +41% (+21% change)
/6
Deviance from PREPANDEMIC trend:
First closure: -27%
First opening: +27% (+54% change)
Second closure: +20% (-7% change)
Second opening: +41% (+21% change)
/6
It seems to me that this data shows that during school closures, typically, there are less referrals for urgent mental health services. And during periods of school opening, the referrals for urgent mental health services rises, on top of a background trend of increase.
/7
/7

This also coincides with what we know about PREPANDEMIC trends in NHS referrals - this is the "seasonality" of urgent referrals - with significant decreases seen during Easter, Summer, and Winter Breaks (increases during school months)
/8
/8

So tell me, what do you see then? Is it fair to say that referrals for urgent distress have gone up during the pandemic? I would say this data supports that.
/9
/9
School Closures? well, in the first wave, we saw quite the decrease. This makes sense; it is likely that many services were not sending in many referrals during the pandemic. The Increase following matched the decrease during. This could very well be a "rebound effect."
/10
/10
In the second wave of school closures, there was an easing of urgent referrals once more, and the period of school opening, and with schools open for longer we did not see things improve, in fact, they got worse.
/11
/11
In my mind, this is the continuation of my hypothesis that:
a) the pandemic sucks
b) schools prepandemic AND postpandemic were associated with more childhood stress and urgent referrals
c) pandemic closures have a modest effect, but trending towards a decrease from opening
/12
a) the pandemic sucks
b) schools prepandemic AND postpandemic were associated with more childhood stress and urgent referrals
c) pandemic closures have a modest effect, but trending towards a decrease from opening
/12
Notes:
* this is not peer reviewed research
* this is my excel equivalent of "napkin math", doing my best to create seasonal models without using complex software
* because its a friday night
* and these are imputed (not raw numbers)
* this is not peer reviewed research
* this is my excel equivalent of "napkin math", doing my best to create seasonal models without using complex software
* because its a friday night
* and these are imputed (not raw numbers)
Limitations:
* Correlation isn't causation
* many things occur on "half months" (ie schools opening mar 8 2021, or summer break starting june 26, 2021), so rounding errors are occurring
* I literally used software to get the numbers. It looks right visually, but small diff poss
* Correlation isn't causation
* many things occur on "half months" (ie schools opening mar 8 2021, or summer break starting june 26, 2021), so rounding errors are occurring
* I literally used software to get the numbers. It looks right visually, but small diff poss
* I AM challenging the claims being made that this shows that school closures are the thing causing harm
* challenging a claim is NOT claiming the opposite
* I AM NOT CLAIMING SCHOOL CLOSURES PROTECT KIDS
* challenging a claim is NOT claiming the opposite
* I AM NOT CLAIMING SCHOOL CLOSURES PROTECT KIDS
Alternative hypothesis (on a friday night):
* "lag effect" closures --> more possible round 1 vs 2, parents tend not to ignore serious MH problems
* "noticing effect" openings --> schools often notice NSSI (please do better if calling "serious attempt" though, hope not)
* "lag effect" closures --> more possible round 1 vs 2, parents tend not to ignore serious MH problems
* "noticing effect" openings --> schools often notice NSSI (please do better if calling "serious attempt" though, hope not)
* "trend accelerator" - pandemic exposed weaknesses in failing child MH system. Given NHS expenditure on same this seems a likely and possible co-contributor. I'm betting going mar'10-mar'20 we would see some pretty impressive growth.
*
• • •
Missing some Tweet in this thread? You can try to
force a refresh





