The sim community are leaders in the understanding of psychological safety...but its time we take the theory beyond it's "safe container"...
Expand the way you think about psychological safety by reading our new work in the area!
advancesinsimulation.biomedcentral.com/articles/10.11…
thread...
Expand the way you think about psychological safety by reading our new work in the area!
advancesinsimulation.biomedcentral.com/articles/10.11…
thread...




Psychological safety - a shared belief that the team is safe for interpersonal risk taking – has been a focus for sim facilitators. Giants have shown how psych safety can be fostered in the confines of the simulation space.
journals.lww.com/simulationinhe…
@GetCuriousNow
journals.lww.com/simulationinhe…
@GetCuriousNow
But psychological safety is even more critical in real workplaces. It is central to how teams accomplish complex work, how they learn together, and how they grow.
@AmyCEdmondson @RoisinODonovan4
@AmyCEdmondson @RoisinODonovan4
We wanted to better understand whether there was a link between psych safety in simulation and psych safety in the real working environments...
So...we studied an existing simulation program @GC_Health - years of weekly sims with registrars and nurses.
So...we studied an existing simulation program @GC_Health - years of weekly sims with registrars and nurses.

74 participants completed narrative surveys and we conducted 19 interviews.
We coded all this data using @RoisinODonovan4's powerful framework for psychological safety in healthcare.
academic.oup.com/intqhc/article…
We coded all this data using @RoisinODonovan4's powerful framework for psychological safety in healthcare.
academic.oup.com/intqhc/article…

What did we find???
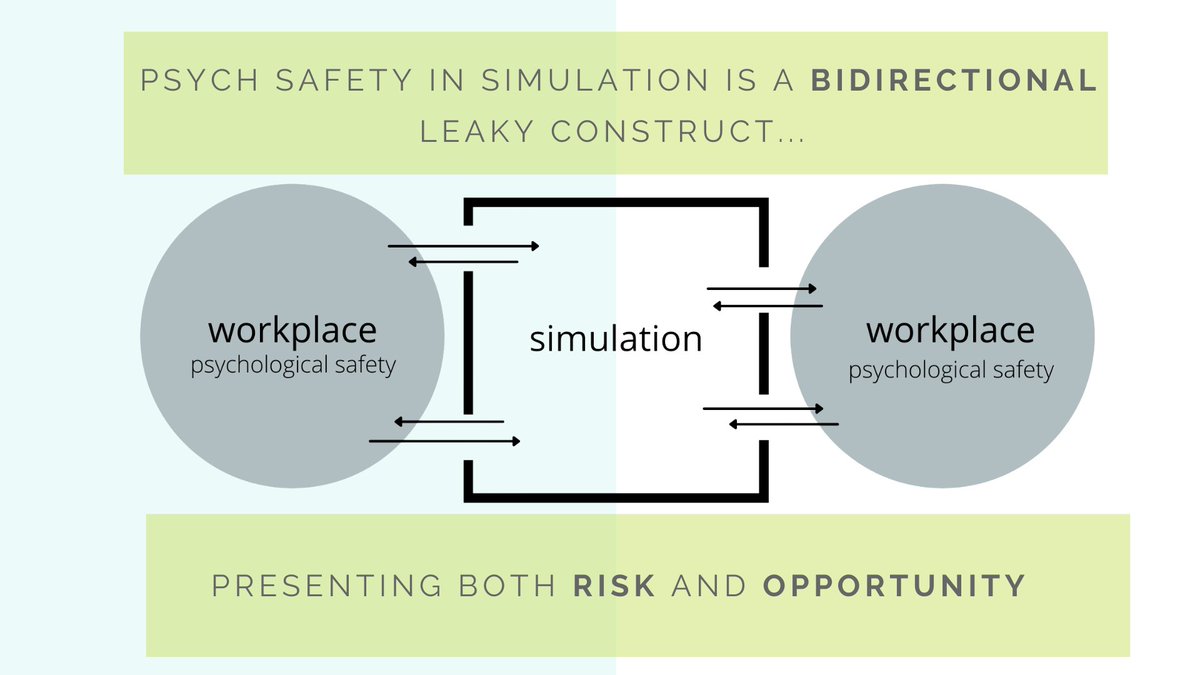
Convincing evidence that workplace psych safety impacts the simulation experience AND experience in simulation impacts workplace psych safety.
Simulation is NOT a safe container...it is a bidirectional leaky construct.
Convincing evidence that workplace psych safety impacts the simulation experience AND experience in simulation impacts workplace psych safety.
Simulation is NOT a safe container...it is a bidirectional leaky construct.

What else did we find?
Simulation was an incubator of familiarity and acted as a magnifying glass on leader behavioral integrity. It was clear that participants viewed simulation as a place where relationships are forged, with both positive and negative consequences.
Simulation was an incubator of familiarity and acted as a magnifying glass on leader behavioral integrity. It was clear that participants viewed simulation as a place where relationships are forged, with both positive and negative consequences.

The implications of the bidirectional nature of psych safety and simulation cannot be understated. It presents both opportunity and risk.
The opportunity - a sacred place to build the magic stuff that makes teams work.
The risk - a frighteningly easy place to destroy it.
The opportunity - a sacred place to build the magic stuff that makes teams work.
The risk - a frighteningly easy place to destroy it.

So...
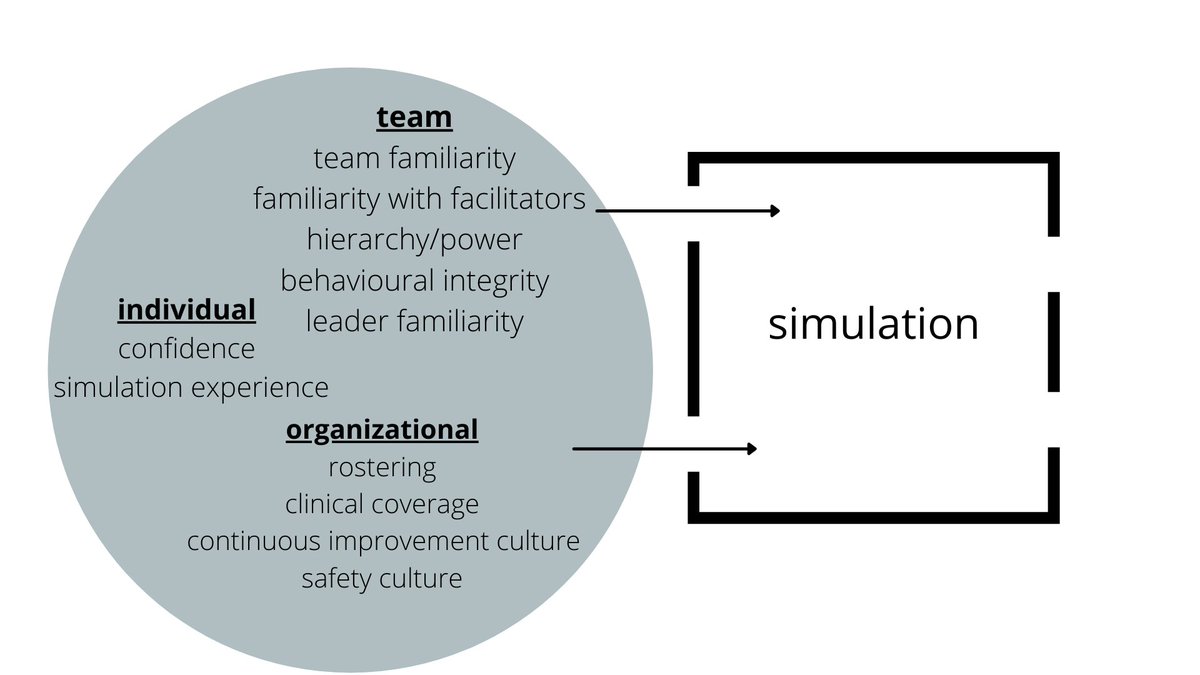
We must be mindful of what leaks INTO the sim space.
Consider the dynamics of the team entering, your relationship with them, and how sim fits in the broader ethos of the organization.
We must be mindful of what leaks INTO the sim space.
Consider the dynamics of the team entering, your relationship with them, and how sim fits in the broader ethos of the organization.

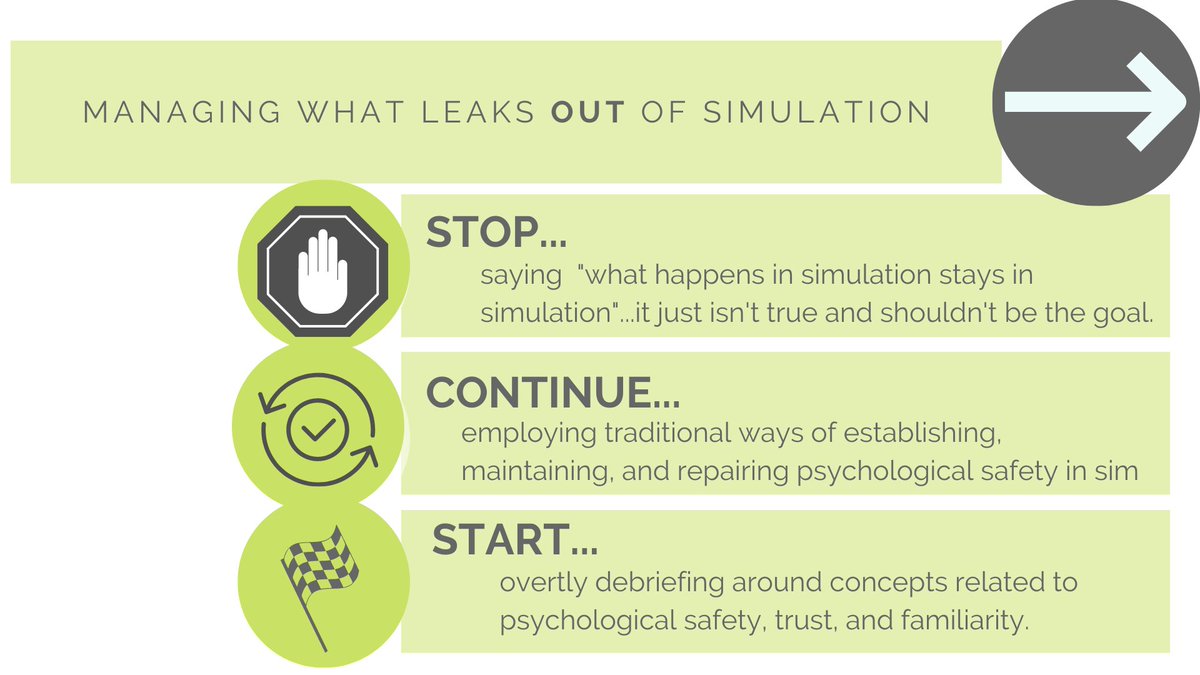
We should also aim to shape what leaks OUT.
STOP saying what happens in simulation stays in simulation...it just isn't true.
Instead aim to make that leak out one of increased psych safety for teams when they head back to work by tailoring your approach and debriefings.
STOP saying what happens in simulation stays in simulation...it just isn't true.
Instead aim to make that leak out one of increased psych safety for teams when they head back to work by tailoring your approach and debriefings.
There's lots more to the story...
Read it all here advancesinsimulation.biomedcentral.com/articles/10.11…
or get in touch with @purdy_eve @socraticEM @WarwickIsaacson
Thanks to @emfresearch @GC_Health @BondUniversity
Read it all here advancesinsimulation.biomedcentral.com/articles/10.11…
or get in touch with @purdy_eve @socraticEM @WarwickIsaacson
Thanks to @emfresearch @GC_Health @BondUniversity

• • •
Missing some Tweet in this thread? You can try to
force a refresh