All you need to know about residual peri-device leaks (PDLs) after LAA occlusion in this 🧵
💢How frequent?
💢Do they matter?
💢What’s their mechanism?
💢Best way to manage?
#CardioTwitter #MedEd #EPeeps
💢How frequent?
💢Do they matter?
💢What’s their mechanism?
💢Best way to manage?
#CardioTwitter #MedEd #EPeeps

How frequent? It depends on how you define PDL!
📌 In PROTECT AF, any PDL at 45d was 41% but ⬇️ to 32% at 1yr (2/3 of leaks ≥3mm)
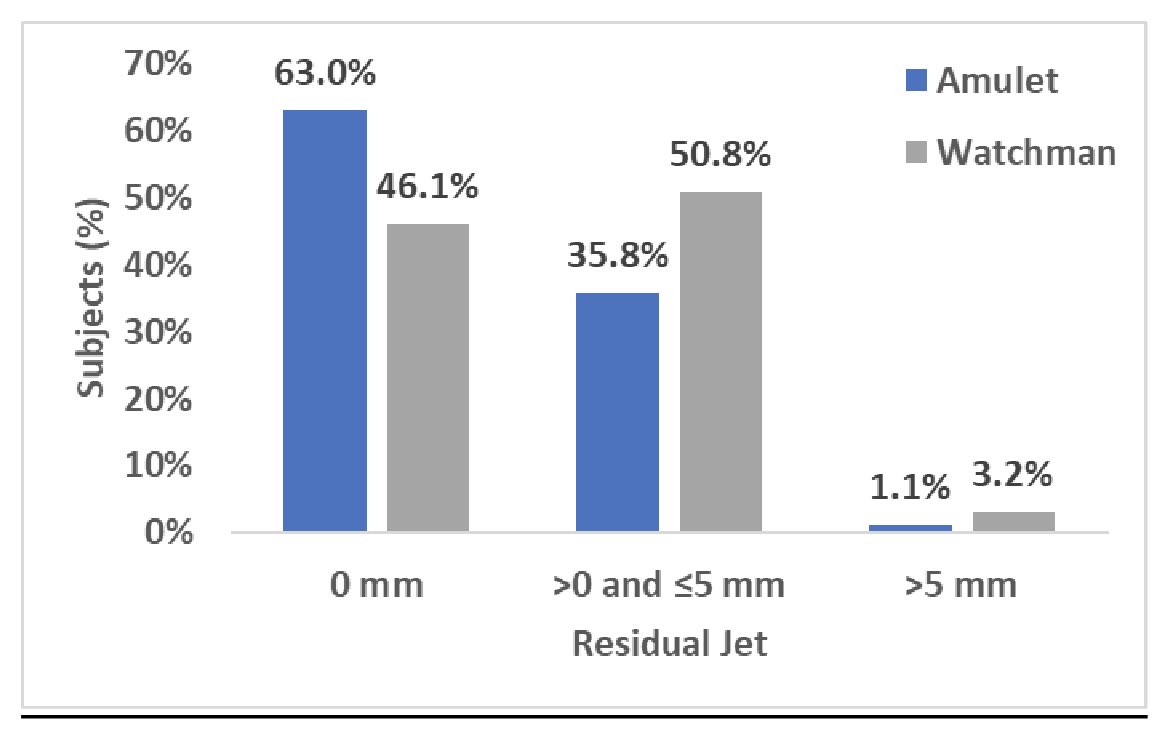
📌 In Amulet IDE, any PDL at 45d was 51% w Watchman & 36% w Amulet
📌 In PINNACLE FLX, any PDL w Watchman FLX was 17% at 45d & ⬇️ to 10.5% at 1yr
📌 In PROTECT AF, any PDL at 45d was 41% but ⬇️ to 32% at 1yr (2/3 of leaks ≥3mm)
📌 In Amulet IDE, any PDL at 45d was 51% w Watchman & 36% w Amulet
📌 In PINNACLE FLX, any PDL w Watchman FLX was 17% at 45d & ⬇️ to 10.5% at 1yr


Do PDLs matter?
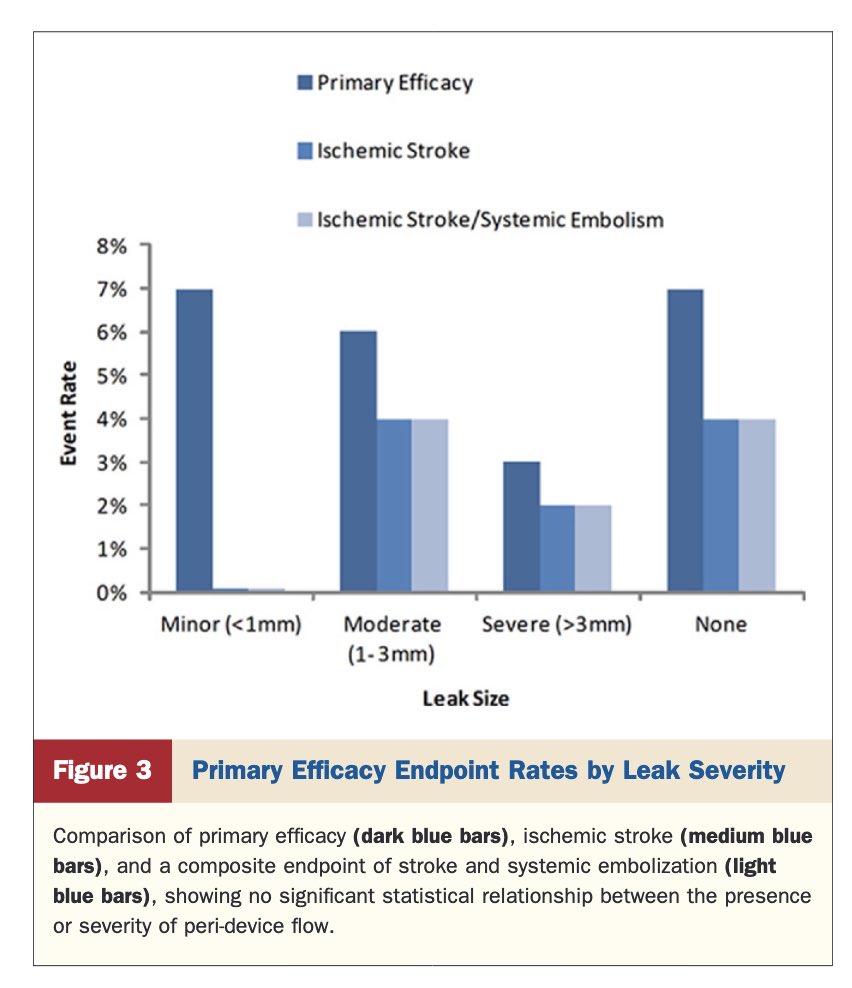
📌 Till recently, we thought they don’t based on early data from PROTECT AF, Amulet registry, etc.
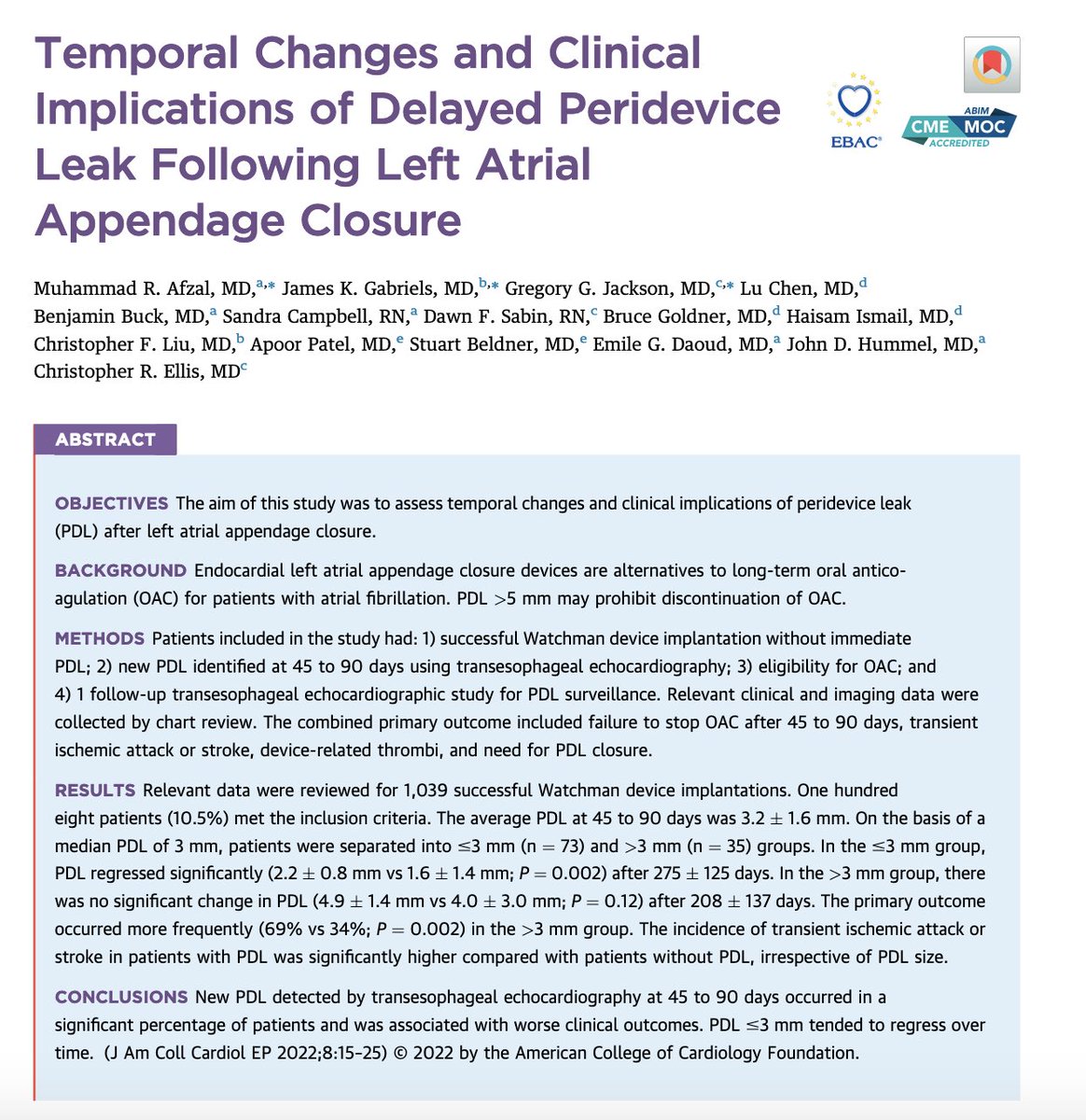
📌 However, data presented at AHA showed that PDLs at 1yr were associated w worse 5yr outcomes
📌@cellisvandyep also recently showed worse outcomes w PDLs
📌 Till recently, we thought they don’t based on early data from PROTECT AF, Amulet registry, etc.
📌 However, data presented at AHA showed that PDLs at 1yr were associated w worse 5yr outcomes
📌@cellisvandyep also recently showed worse outcomes w PDLs


So, do PDL after LAAO really matter?
Stay tuned! & join us for a LBCT/featured research session at ACC on April 3rd.
We will present the largest study on PDL from the NCDR LAAO registry👇
Stay tuned! & join us for a LBCT/featured research session at ACC on April 3rd.
We will present the largest study on PDL from the NCDR LAAO registry👇

🔑 question:
What’s the mechanism of PDL?
📌Currently we arbitrarily group all leaks together as one entity
📌However, there are several mechanisms as shown👇
📌Clinical implications & management of PDL are likely related to their mechanism (small edge leak vs uncovered lobe)
What’s the mechanism of PDL?
📌Currently we arbitrarily group all leaks together as one entity
📌However, there are several mechanisms as shown👇
📌Clinical implications & management of PDL are likely related to their mechanism (small edge leak vs uncovered lobe)

How to best manage PDLs?
Reported solutions:
📌 Stay on OAC
📌 Plugs
📌 Double occluders
📌 Coils
But, only short-term data available.
My take; an ounce of prevention is worth a pound of cure.
Efforts should l focus on mitigation; new devices & steerable sheath might help
Reported solutions:
📌 Stay on OAC
📌 Plugs
📌 Double occluders
📌 Coils
But, only short-term data available.
My take; an ounce of prevention is worth a pound of cure.
Efforts should l focus on mitigation; new devices & steerable sheath might help


Final thoughts 💭
💢Leaks after LAAO are common
💢Data on clinical significance are conflicting (but more coming)
💢Definitions controversial (size vs mechanism, what size?)
💢Management challenging:
- OAC =🩸
- Plugs/coils = no long-term data
💢Mitigation strategies needed
💢Leaks after LAAO are common
💢Data on clinical significance are conflicting (but more coming)
💢Definitions controversial (size vs mechanism, what size?)
💢Management challenging:
- OAC =🩸
- Plugs/coils = no long-term data
💢Mitigation strategies needed
• • •
Missing some Tweet in this thread? You can try to
force a refresh