Small thread 🧵illustrating #POCUS based hemodynamic assessment. Relatively a classic case of pulmonary HTN and right heart failure but would like to get some insights from the experts.
1/ Parasternal long axis (PSAX) showing D-sign
#VExUS #MedEd #Nephpearls #IMPOCUS
1/ Parasternal long axis (PSAX) showing D-sign
#VExUS #MedEd #Nephpearls #IMPOCUS
2/ Parasternal long axis (PLAX) view demonstrating RV dilatation.
One of the three musketeers is big. Don't know what I'm talking about? Here is a brief reminder: 🔗nephropocus.com/2021/07/12/the…
(Mobile thing in the RVOT is PA catheter; M-mode quiz from this morning is actually this)
One of the three musketeers is big. Don't know what I'm talking about? Here is a brief reminder: 🔗nephropocus.com/2021/07/12/the…
(Mobile thing in the RVOT is PA catheter; M-mode quiz from this morning is actually this)
3/ Apical 4-chamber view #POCUS
Note how RV is dilated - bigger than LV and forming the cardiac apex.
Inter-atrial septum is bowing to the left indicating high right atrial pressure (not unexpected).
Note how RV is dilated - bigger than LV and forming the cardiac apex.
Inter-atrial septum is bowing to the left indicating high right atrial pressure (not unexpected).
4/ Apical 4C color showing tricuspid regurgitation. At least moderate qualitatively. Will show a TR jet obtained using pulsed wave Doppler in subsequent tweets.
#echofirst
#echofirst
5/ Subxiphoid SAX showing D-sign #echofirst
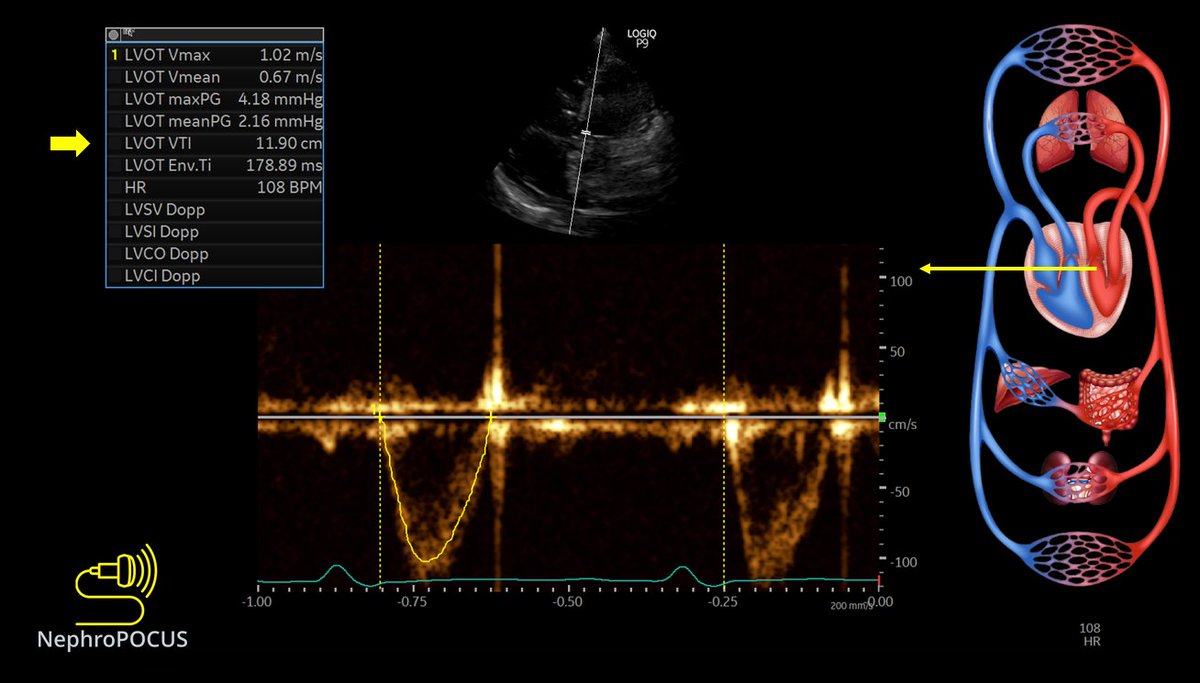
6/ LV systolic function appears to be decreased but lets check LVOT VTI (left ventricular outflow tract velocity time integral), which is used to estimate stroke volume. Normally, it's ~18-22 cm
Here its ⬇️
Here its ⬇️
7/ RVOT VTI (right ventricular outflow tract VTI). It is generally slightly ⬇️ than LVOT VTI. Essentially everything that goes through right side should come out through the left so the stroke volume should be the same (RVOT diameter is bigger than LVOT, more so in this case)

8/ RVOT Doppler also gives a clue about the severity of pulmonary hypertension.
Compare the shape of 👆with 👇 #POCUS
Compare the shape of 👆with 👇 #POCUS

9/ RVOT continuous wave (CW) Doppler👇
Remember PW Doppler helps to measure velocity at a particular location while CW helps to measure gradient across something (valve). From this, we get an idea of pulmonary artery diastolic pressure.
Doppler basics: 🔗renalfellow.org/2020/12/07/bas…
Remember PW Doppler helps to measure velocity at a particular location while CW helps to measure gradient across something (valve). From this, we get an idea of pulmonary artery diastolic pressure.
Doppler basics: 🔗renalfellow.org/2020/12/07/bas…

10/ Next RVSP (right ventricular systolic pressure) - it is obtained by CW Doppler across the tricuspid valve and adding right atrial pressure (based on IVC).
In this case, IVC was plethoric, so RAP presumed to be 15 mmHg.
estimated RVSP = ~36 + 15 = 51 mmHg. #POCUS
In this case, IVC was plethoric, so RAP presumed to be 15 mmHg.
estimated RVSP = ~36 + 15 = 51 mmHg. #POCUS

11/ Now coming to the effects of RAP, that is your favorite part, #VExUS
First is IVC - appears plethoric, hepatic veins are distended
Estimated RAP at least 15 mmHg
First is IVC - appears plethoric, hepatic veins are distended
Estimated RAP at least 15 mmHg


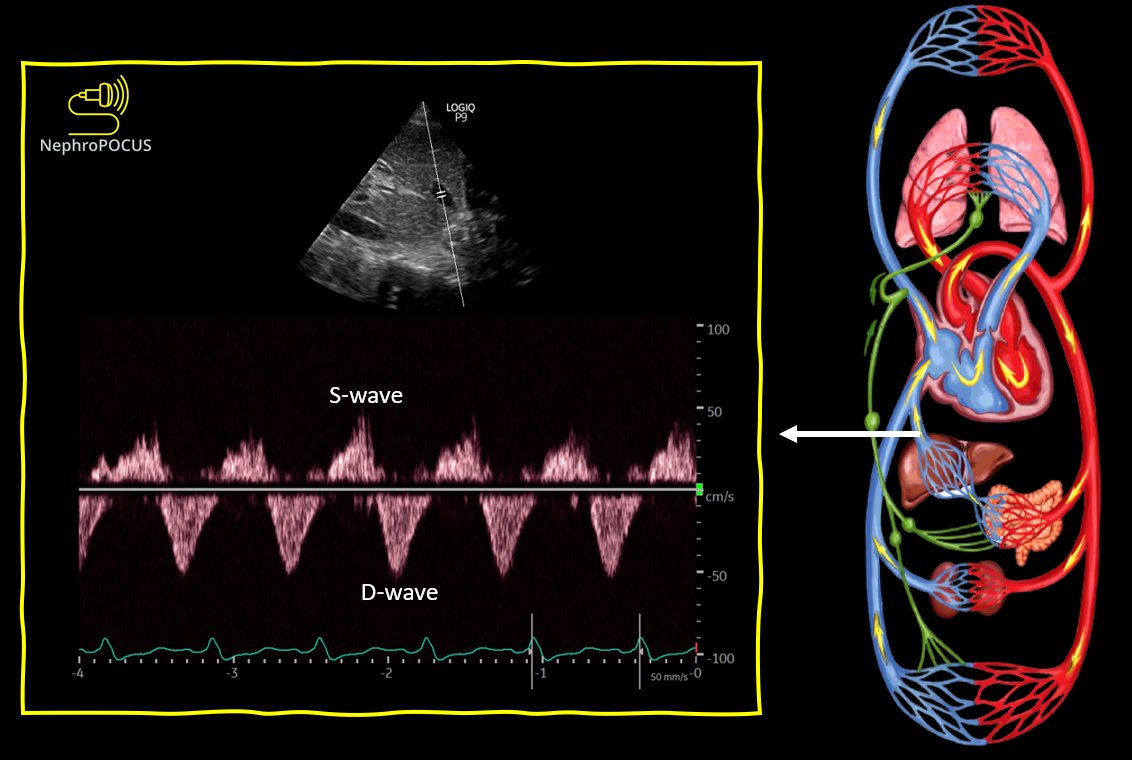
14/ Intra-renal vein #VExUS - D-only pattern suggestive of congestive nephropathy.
As @ThinkingCC says, organs don't care whether the congestion is due to pressure or volume.
Notably, this pattern is associated with worse prognosis in patients with pulmonary hypertension.
As @ThinkingCC says, organs don't care whether the congestion is due to pressure or volume.
Notably, this pattern is associated with worse prognosis in patients with pulmonary hypertension.

Tagging some hemodynamic experts. Have some questions below.
@khaycock2 @MDBeni @IM_Crit_ @Thind888 @msiuba @siddharth_dugar @katiewiskar @ArgaizR @RJonesSonoEM @IMPOCUSFocus
@khaycock2 @MDBeni @IM_Crit_ @Thind888 @msiuba @siddharth_dugar @katiewiskar @ArgaizR @RJonesSonoEM @IMPOCUSFocus
First, some details I omitted above.
1. Pt was on dobutamine and Treprostinil at the time of #POCUS
2. Had right heart cath from the same day (2 hours prior to this + leave-in pulmonary catheter)
1. Pt was on dobutamine and Treprostinil at the time of #POCUS
2. Had right heart cath from the same day (2 hours prior to this + leave-in pulmonary catheter)
Q1. Pt has precapillary pulmonary hypertension - pulmonary vascular resistance 7.9 Wood units. Aren't we expected to see notching on RVOT Doppler? Current pattern appears triangular, which is not normal but does it look bad?
Pulmonary pressure at the time of scan 64/30.
Pulmonary pressure at the time of scan 64/30.
#POCUS underestimating pulm pressures? 🤔 Tried to align with the jet but not 💯sure.
Q2: Since this patient chronically has RV dilatation and presumably plethoric IVC, we do not want to aggressively ultrafiltrate if dialysis is needed. What is 'cautious ultrafiltration'?
Q2: Since this patient chronically has RV dilatation and presumably plethoric IVC, we do not want to aggressively ultrafiltrate if dialysis is needed. What is 'cautious ultrafiltration'?
If I don't have invasive monitoring available (once moved out of ICU), how would I know what is the right amount of fluid to remove?
Feel free to comment/educate on any of the above images. Thank you 🙏
Oh forgot, I didn't measure TAPSE but tricuspid annulus seems to be moving OK. You think its because of inotrope/pulmonary vasodilator? Is it necessary to have low TAPSE or S' in RV failure like this?
• • •
Missing some Tweet in this thread? You can try to
force a refresh