
True. It only prevented death (3 vs 10) and ICU admission (4 vs 10). But who cares about that if it doesn't prevent... (*checks notes*) drop in O2 levels below 95%?
Did anyone claim it did that?
Read the results of the study yourselves and then the conclusions... 🙄
Did anyone claim it did that?
Read the results of the study yourselves and then the conclusions... 🙄
https://twitter.com/NAChristakis/status/1494772663356641290

Some required reading for all those playing with words like "statistically significant" without any understanding that those words have a specific technical meaning that is not the same thing as what we mean by "significant" in everyday life.
nature.com/articles/d4158…
nature.com/articles/d4158…
The trial had decent dosing and recommended taking the medicine with a meal, which is good practice. On the minus side, people were enrolled 5.1 days after symptoms. Which means the average patient would've been excluded from the Paxlovid & Molnupiravir trials for being too late.
Study investigated if ivm prevents progression to severe disease. (under 95% O2)
Patients were enrolled, on average 5.1 days from symptom onset (quite late)
Treatment was over 5 days
Treatment group progressed to severe disease in 3.2 days
(i.e. before treatment complete)
🙄
Patients were enrolled, on average 5.1 days from symptom onset (quite late)
Treatment was over 5 days
Treatment group progressed to severe disease in 3.2 days
(i.e. before treatment complete)
🙄
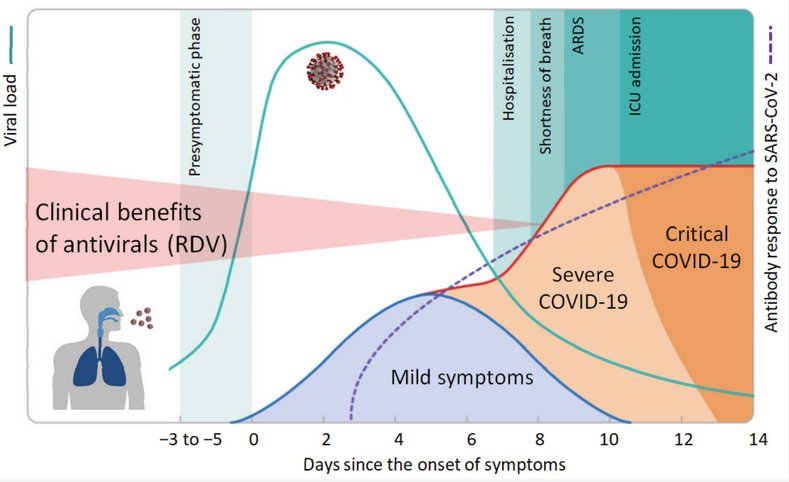
And a reminder what "average 5.1 days since onset of symptoms" means for investigating an antiviral drug.
• • •
Missing some Tweet in this thread? You can try to
force a refresh







