
What went wrong with the recent I-TECH Ιvermectin study published in JAMA?🧵
In brief, the study design was such that any other antiviral, such as Paxlovid or Molnupiravir, would also have failed.
This thread will explain why.
jamanetwork.com/journals/jamai…
In brief, the study design was such that any other antiviral, such as Paxlovid or Molnupiravir, would also have failed.
This thread will explain why.
jamanetwork.com/journals/jamai…
Briefly, an antiviral started avg 5.1 days after symptom onset, with a primary endpoint that is triggered 3.1 days after start of treatment, when treatment is for 5 days, will be almost impossible to show benefit.
The avg patient didn't even have time to complete the treatment.
The avg patient didn't even have time to complete the treatment.

In the case of Paxlovid, the average patient in this trial would not even have been eligible to receive Paxlovid, since they would have been deemed "too late". fda.gov/media/155050/d…

In the case of Molnupiravir, the exact same thing is true. The average patient in this trial would not be eligible to even receive it at all. theatlantic.com/health/archive…
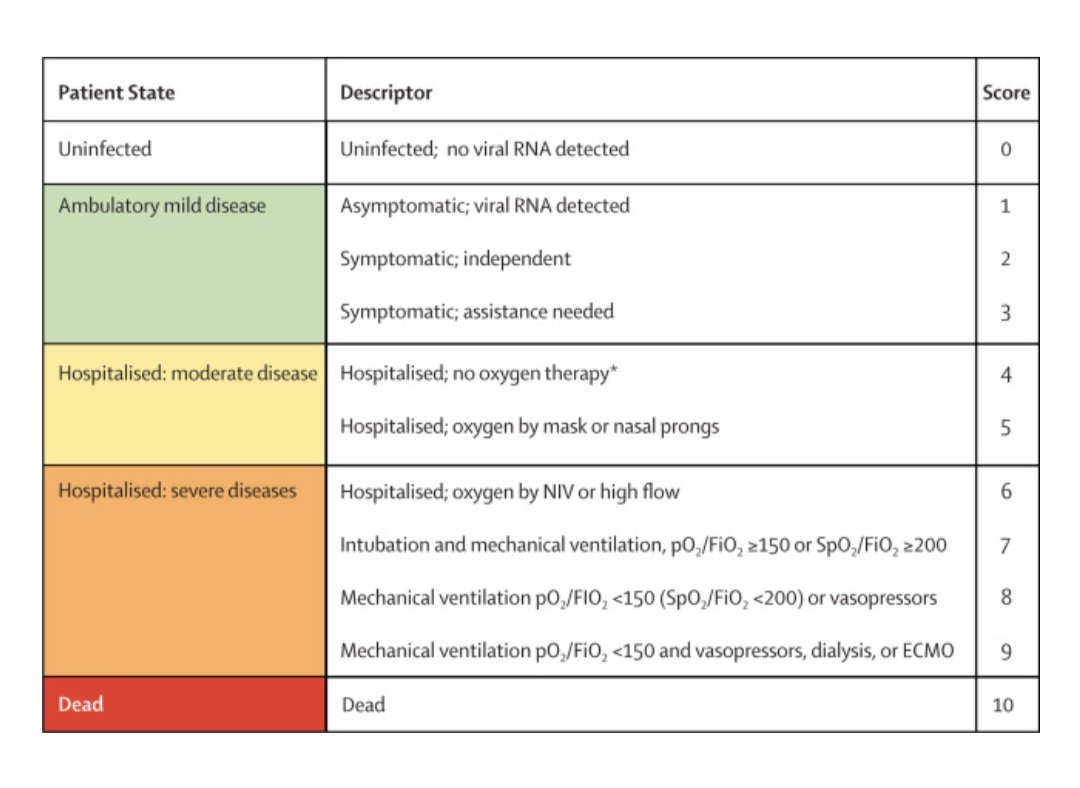
Interestingly, the authors call the endpoint "severe disease" and cite the following WHO paper:
thelancet.com/journals/lanin…
thelancet.com/journals/lanin…
The paper, however, classifies "Severe Disease" as stage 5 and below, whereas the WHO defines "Severe Disease" as stages 6 and below. Why play with definitions this way?
https://twitter.com/compsciman/status/1494905161709498368?s=20&t=ap6i70aMEppS3f-dVQtiRw
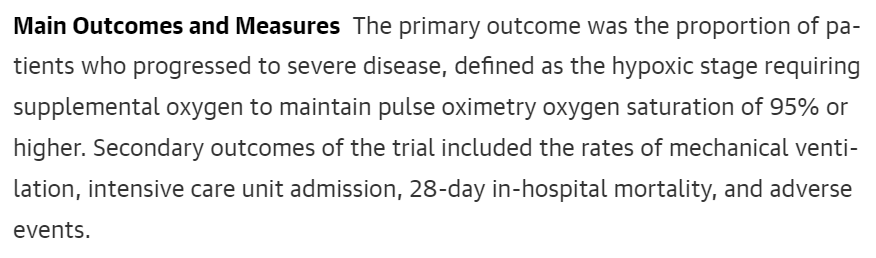
Also the primary endpoint is worded is such that clinical judgement comes into play:
"patients requiring supplemental oxygen to maintain pulse oximetry oxygen saturation of 95% or higher"
They could have used "patients who measured oximetry oxygen saturation of 95%" but didn't.
"patients requiring supplemental oxygen to maintain pulse oximetry oxygen saturation of 95% or higher"
They could have used "patients who measured oximetry oxygen saturation of 95%" but didn't.
Putting it all together, the patients were enrolled way too late for an antiviral, and the primary endpoint was such that it triggered before the treatment was complete. There was also human judgement involved, which isn't a good thing, *especially in an open-label trial*.
When we look at the hard endpoints, such as requiring mechanical ventilation and death, what do we see?
Not only do these endpoints look incredibly positive for the Ιvermectin group, but they are also the strongest (p-value) findings of the paper.
Not only do these endpoints look incredibly positive for the Ιvermectin group, but they are also the strongest (p-value) findings of the paper.

As for my position on Ιvermectin, it's been consistent since the summer. We don't know if it works or not because *appropriately sized studies with correct dosing and timing* aren't being done. But it's safe enough that it's not worth not giving.
https://twitter.com/alexandrosM/status/1432247947601661952
You can see a prior review of the evidence I did a couple of months back here, showing that there is a clear, if uncertain, signal of efficacy. doyourownresearch.substack.com/p/a-conflict-o…
The real scandal is that the proper authorities don't seem interested in drugs like this, or even fluvoxamine, which has even stronger data.
Run a trial with the same parameters as Paxlovid or Molnupiravir. It can't be impossible, it's been already done for those medicines.
Run a trial with the same parameters as Paxlovid or Molnupiravir. It can't be impossible, it's been already done for those medicines.
• • •
Missing some Tweet in this thread? You can try to
force a refresh






