
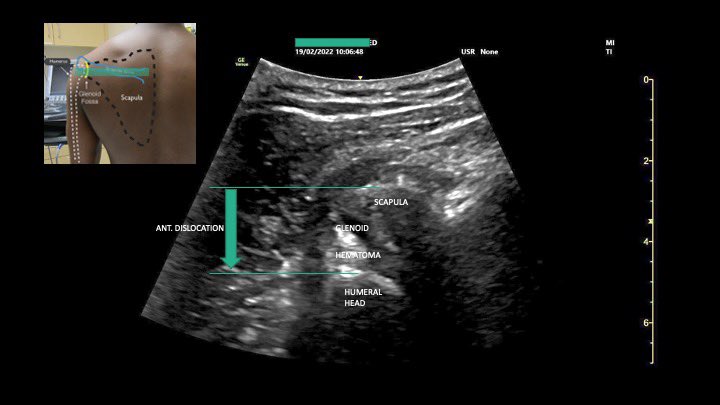
Thread: 1/3 Clinically anterior glenohumeral dislocation, confirmed by #POCUS within 5 min of arrival 
2/3 Pain 10/10 to 0/10 within 5 min of interscalene block
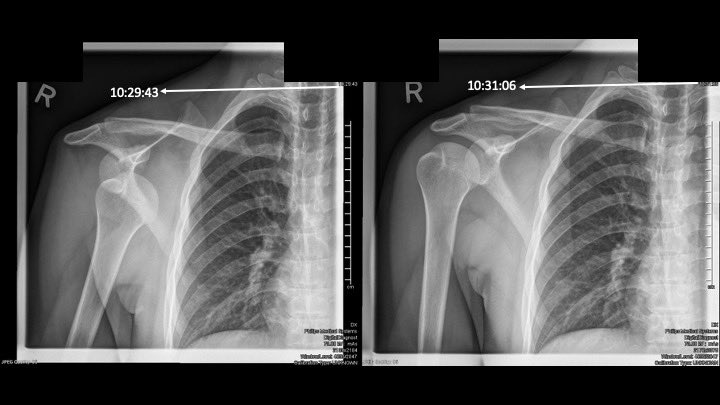
3/3 X-ray was required for followup purposes. Patient walked to x-ray comfortably, and reduced in x-ray suite painlessly and effortlessly. ED LoS 40 min.
@threadreaderapp unroll please
• • •
Missing some Tweet in this thread? You can try to
force a refresh




