1/n #POCUS M/68, vomiting since 6 hours, back pain since 1 h. Says no to chest pain /abd pain / dyspnea. Diaphoretic, vomiting, HR 90, RR 24, BP 128/70, SpO2 91% (air). Reduced BS left side, Abd distended, nontender. ECG normal. Is it acute aortic? Tried to get PLAX heart -
2/n - scanning right parasternal area - found the heart - hyperdynamic, but nothing grossly wrong there.
3/n #POCUS Another look at left hemithorax anteriorly (parasaggital plane, mid-clavicular line, 4th. ICS)
4/n Scanning left hemithorax long axis cranial-caudal slide 3rd ICS ant axillary - looks like eventration of left hemidiaphragm with distended stomach below it
5/n scanning abdomen - features of small bowel obstruction. Dilated jenunal loop in near field, with bidirectional peristalsis, and dilated ileum in far field
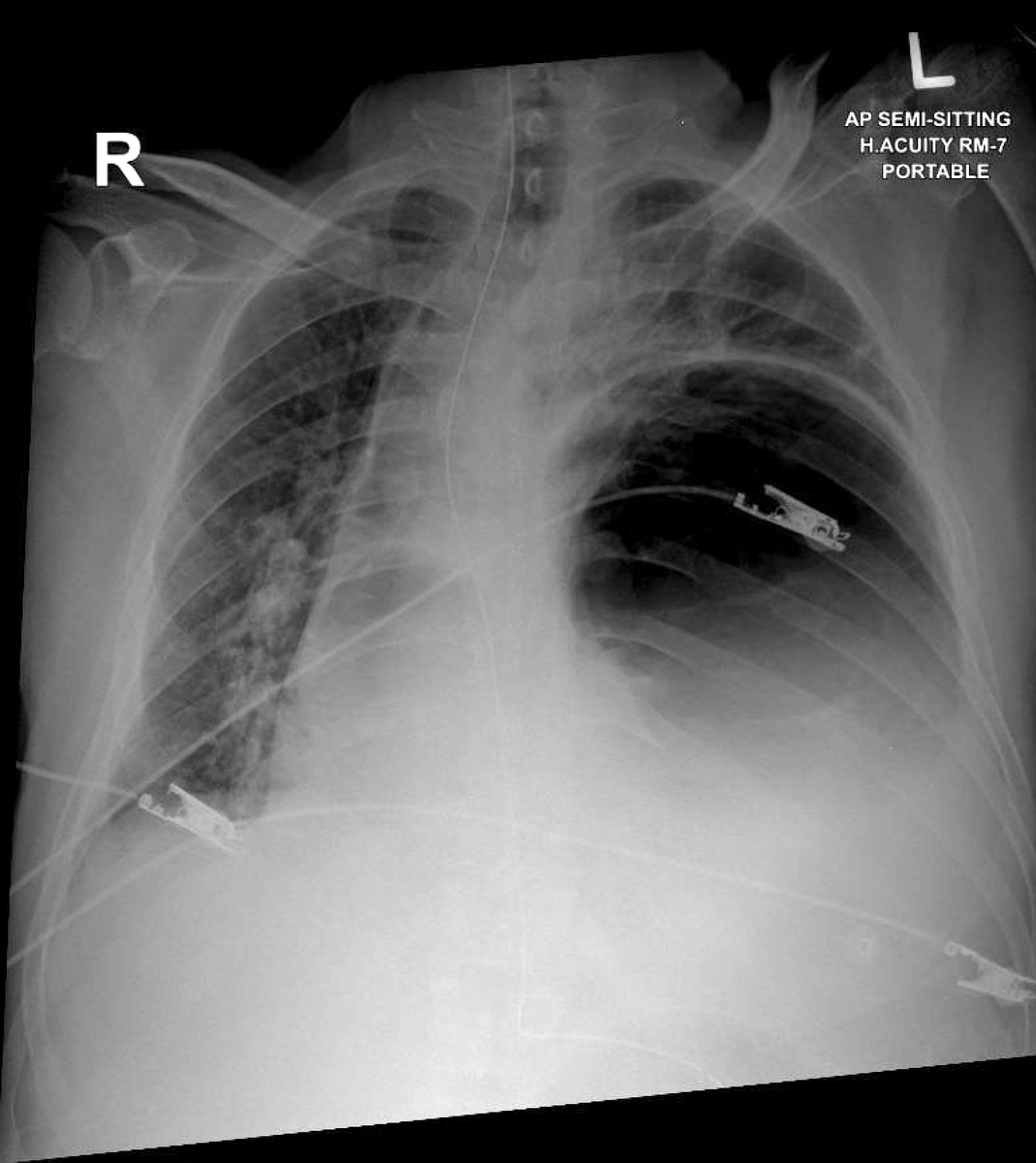
6/n - all of the above within 10 min of patient arrival. Proceeded to insert NGT, called for portable CXR
- no surprise.
- no surprise.
7/n - surgical colleagues at bedside, pt taken for surgery (via CT)
8/8 - Surgery: terminal ileum stricture obstructed by a phytobezoar. Resection/anastomosis, SICU, extubated at 48 h, doing well.
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh