New embarrassingly bad study of ivermectin is a textbook example of “confounding by indication”
In short a retroactive database review found that people w/ COVID did worse if given remdesivir (only given to sick inpatients) than ivermectin (only given to well outpatients)🤔
1/
In short a retroactive database review found that people w/ COVID did worse if given remdesivir (only given to sick inpatients) than ivermectin (only given to well outpatients)🤔
1/

There are many problems with this “study”.
First it’s generous to even call it a “study.” It’s an *abstract* of a retrospective database review. The whole “article” is less than a page (see below).
It wasn’t pre-registered.
sciencedirect.com/science/articl…
2/
First it’s generous to even call it a “study.” It’s an *abstract* of a retrospective database review. The whole “article” is less than a page (see below).
It wasn’t pre-registered.
sciencedirect.com/science/articl…
2/

The methods are weird.
They found 1.7 million people w/ COVID. Out of this group they identified 1,072 who received ivermectin (not exactly widely used) & 40k who received remdesivir
The groups were very dissimilar: IVM was 10 yrs younger. They don’t report any comorbidities
3/
They found 1.7 million people w/ COVID. Out of this group they identified 1,072 who received ivermectin (not exactly widely used) & 40k who received remdesivir
The groups were very dissimilar: IVM was 10 yrs younger. They don’t report any comorbidities
3/

Despite the groups being wildly dissimilar, they *somehow* adjusted for potential compounders. (They don’t say how)
Crucially they did NOT adjust for hospitalization status. This means they compared COVID outpatients (on IVM) to COVID inpatients (on remdesivir). 🍎to🍊
4/
Crucially they did NOT adjust for hospitalization status. This means they compared COVID outpatients (on IVM) to COVID inpatients (on remdesivir). 🍎to🍊
4/
The authors are interesting…
The first two are medical students, the 3rd is a plastic surgery resident.
(Nothing wrong with this, though it is weird for the MS not to be affiliated w/ SOM)
The fifth & sixth authors are plastic surgeons. Neither has expertise in ID or COVID
5/
The first two are medical students, the 3rd is a plastic surgery resident.
(Nothing wrong with this, though it is weird for the MS not to be affiliated w/ SOM)
The fifth & sixth authors are plastic surgeons. Neither has expertise in ID or COVID
5/
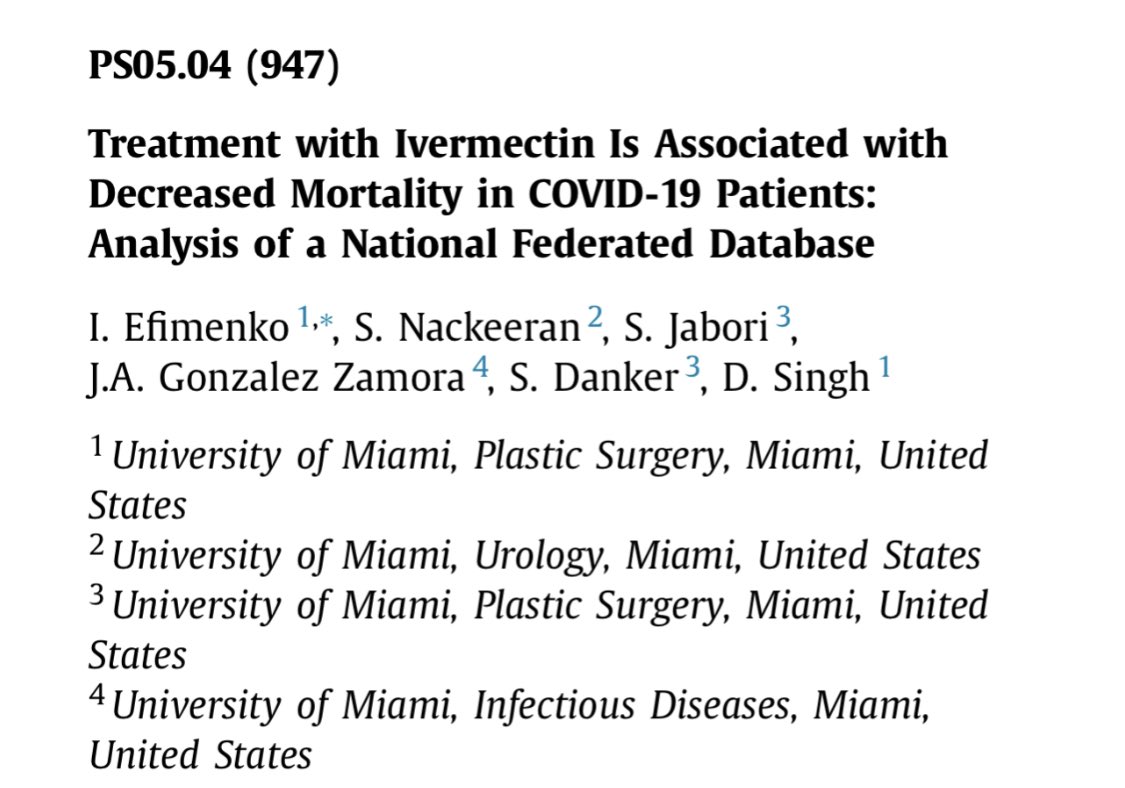
The 4th author @JoseGonzalesZa1 is the head of the ID fellowship at UMiami. He is an actual expert on this topic.
Based on his other work, I’m pretty sure he doesn’t think ivermectin is an effective therapy as this abstract concludes. See translation of one of his articles👇
6/
Based on his other work, I’m pretty sure he doesn’t think ivermectin is an effective therapy as this abstract concludes. See translation of one of his articles👇
6/




All of this makes me wonder - did the authors all even read/approve this abstract?
Did the peer reviewers think it was odd that plastic surgeons were doing research on ivermectin for COVID?
7/
Did the peer reviewers think it was odd that plastic surgeons were doing research on ivermectin for COVID?
7/
I wonder if this abstract was the work of an eager group of students/residents who were inadequately supervised by more experienced researchers
That seems like the only way to explain such an obvious confounder being missed
This must have slipped past peer review at #IMED21
8/
That seems like the only way to explain such an obvious confounder being missed
This must have slipped past peer review at #IMED21
8/

Bottom line:
-this abstract of a retrospective review is fatally flawed due to the confounder of hospitalization (+more). There is no evidence that ivermectin reduces mortality
-it won’t stop fringe docs cashing in on selling ivermectin from promoting this “massive study”
9/9
-this abstract of a retrospective review is fatally flawed due to the confounder of hospitalization (+more). There is no evidence that ivermectin reduces mortality
-it won’t stop fringe docs cashing in on selling ivermectin from promoting this “massive study”
9/9

• • •
Missing some Tweet in this thread? You can try to
force a refresh