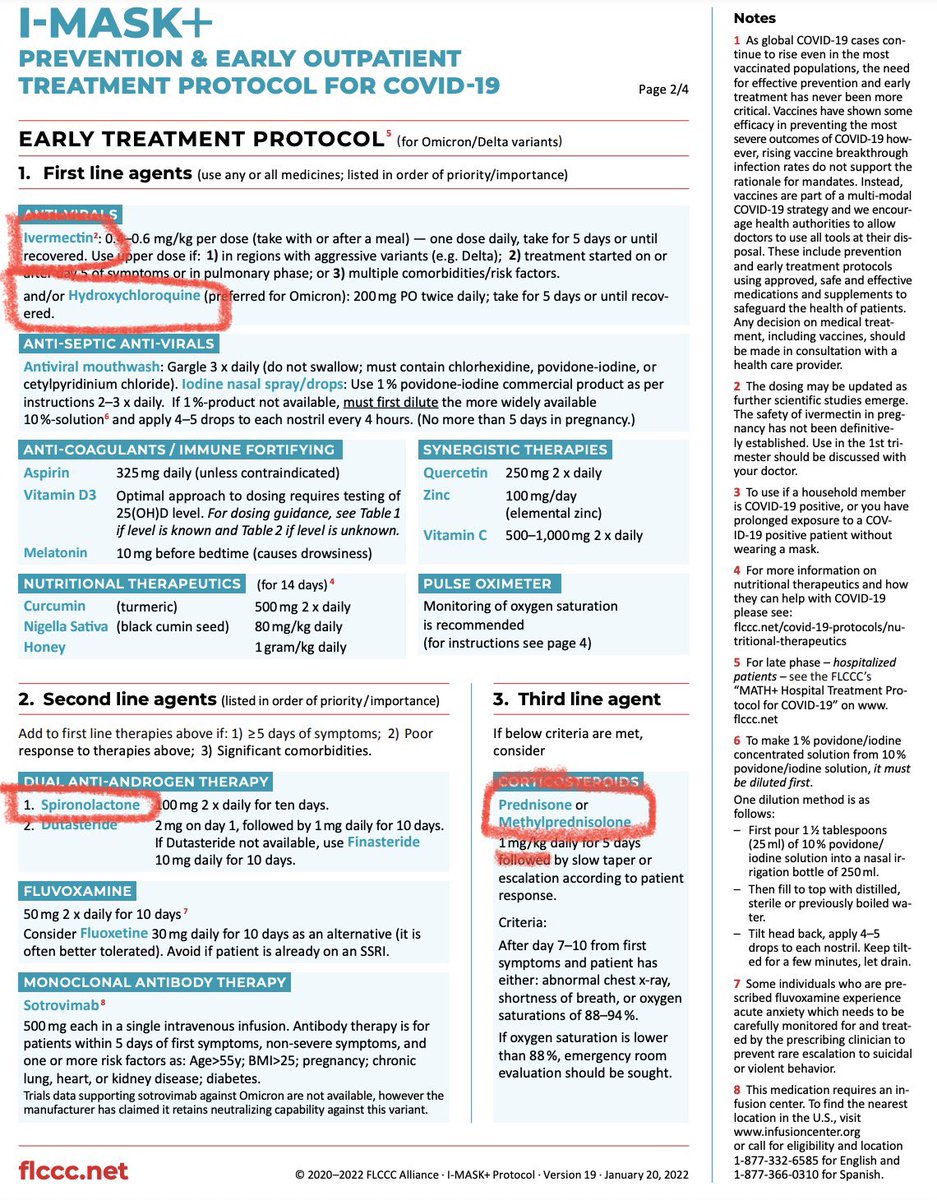
The FLCCC’s “data analyst” (who has no pharm training) is dosing ivermectin horse paste
Only problem: he makes a FATAL math error
A tube of horse paste contains 6gm (6080 mg) of ivermectin at a concentration of 18.7 mg/ml
@TwitterSafety suspend this guy before he kills someone
Only problem: he makes a FATAL math error
A tube of horse paste contains 6gm (6080 mg) of ivermectin at a concentration of 18.7 mg/ml
@TwitterSafety suspend this guy before he kills someone
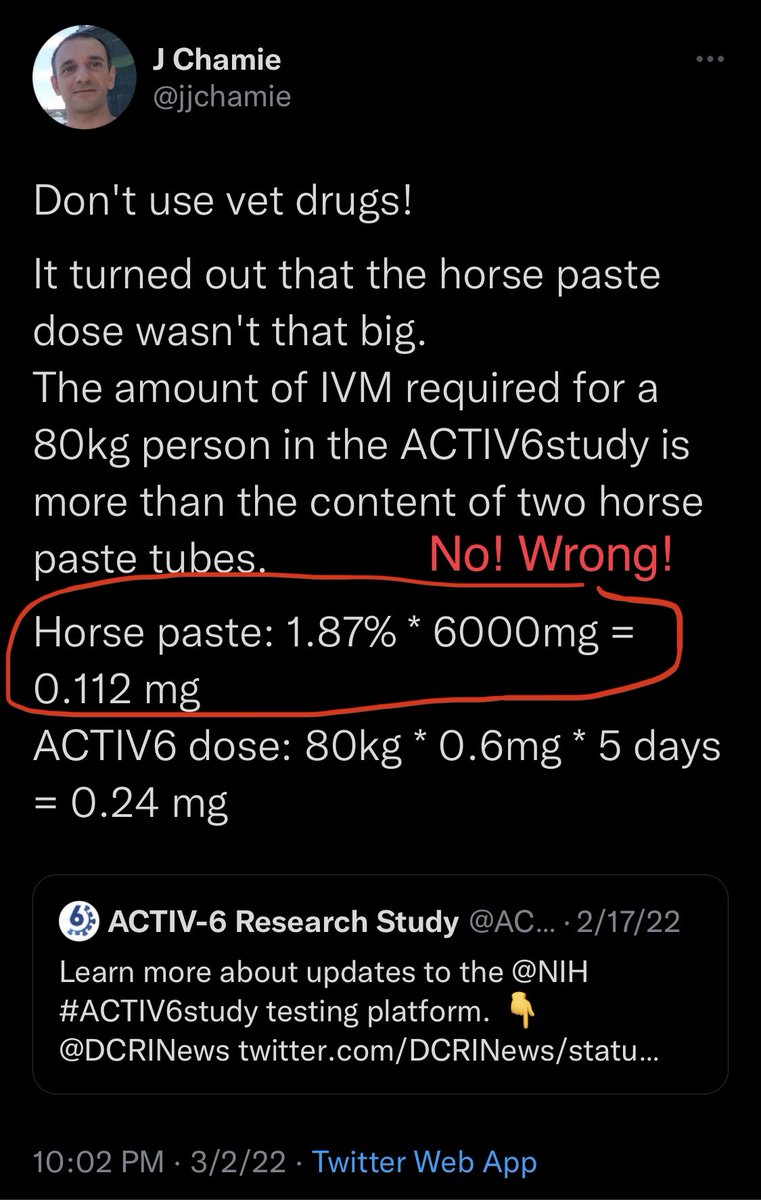

This guy actually got both calculations completely wrong.
In the ACTIV6 trial an 80 kg person receiving 0.6 mg/kg of ivermectin would receive:
80 kg * 0.6 mg/kg = 48 mg per day
(Somehow he calculated 0.24 mg so he was off by 200x; another huge error 😱)
In the ACTIV6 trial an 80 kg person receiving 0.6 mg/kg of ivermectin would receive:
80 kg * 0.6 mg/kg = 48 mg per day
(Somehow he calculated 0.24 mg so he was off by 200x; another huge error 😱)
Bottom line:
- don’t take animal meds EVER; it’s very easy to make a fatal mistake
- don’t take medical advice from a guy with zero training who can’t multiply two numbers correctly
- don’t take animal meds EVER; it’s very easy to make a fatal mistake
- don’t take medical advice from a guy with zero training who can’t multiply two numbers correctly
I deleted a fourth tweet in this series because I made a math error. This is a great reminder of why pharmacists are absolutely life saving!
• • •
Missing some Tweet in this thread? You can try to
force a refresh