
Pandemic Mistakes
Part 3 of 10
One of the worst pandemic mistakes, IMO:
In the UK in April 2020, a nationwide directive to ration oxygen was issued.
Rationing oxygen, in the UK!
🧵
#PandemicMistakes
Part 3 of 10
One of the worst pandemic mistakes, IMO:
In the UK in April 2020, a nationwide directive to ration oxygen was issued.
Rationing oxygen, in the UK!
🧵
#PandemicMistakes
A bit of background:
1. For the vast majority of Covid patients, the lower part of the lungs are unaffected. Most symptoms come from the infection in the upper airways, but don't affect our ability to absorb oxygen.
2. Severe Covid is defined as the requirement for oxygen...
1. For the vast majority of Covid patients, the lower part of the lungs are unaffected. Most symptoms come from the infection in the upper airways, but don't affect our ability to absorb oxygen.
2. Severe Covid is defined as the requirement for oxygen...
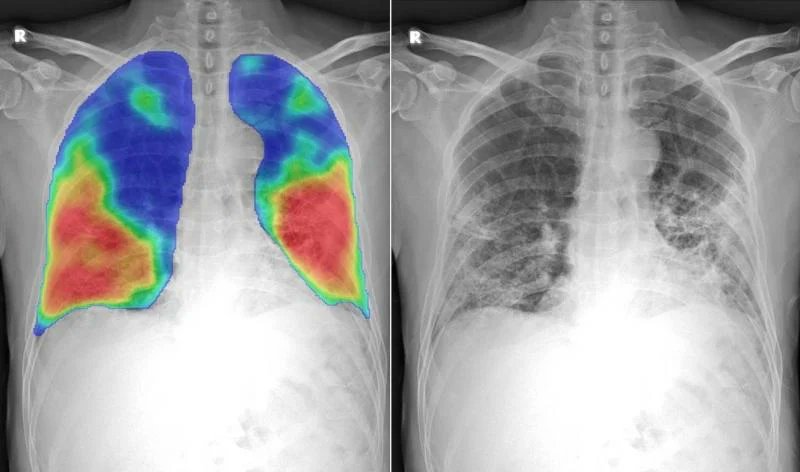
...this means the lower lungs are affected.
[Picture shows Severe Covid. Unique pattern in the very lower parts of the lungs. The red = inflamed. Blue = normal. Where it is red, the ability to transfer oxygen into the blood is reduced]
[Picture shows Severe Covid. Unique pattern in the very lower parts of the lungs. The red = inflamed. Blue = normal. Where it is red, the ability to transfer oxygen into the blood is reduced]
If enough lung is inflamed, then our blood oxygen levels will start to decrease. This is called hypoxia (low blood oxygen).
Hypoxia leads to tissue damage, increases the risk of clotting, and worsens inflammation.
Hypoxia leads to tissue damage, increases the risk of clotting, and worsens inflammation.
If hypoxia worsens further and is not corrected, then death or disability occurs due usually to heart and/or brain damage.
Normal (healthy) oxygen levels are between 96 to 98%.
We normally administer oxygen if oxygen levels fall below 95%.
brit-thoracic.org.uk/quality-improv…
Normal (healthy) oxygen levels are between 96 to 98%.
We normally administer oxygen if oxygen levels fall below 95%.
brit-thoracic.org.uk/quality-improv…
On April 9th 2020, NHS England issued a directive to reduce oxygen targets nationwide.
Overnight we went from admitting all hypoxic patients to admitting only the more severely hypoxic patients.
madeinheene.hee.nhs.uk/Portals/0/Clin…
Overnight we went from admitting all hypoxic patients to admitting only the more severely hypoxic patients.
madeinheene.hee.nhs.uk/Portals/0/Clin…
A couple of points about the directive:
1. It was nationwide.
2. It applied to all conditions, not just Covid.
3. It was issued NOT due to oxygen shortages but due to concerns the oxygen pipes would not be able to handle the increased flow of oxygen in some hospitals.
1. It was nationwide.
2. It applied to all conditions, not just Covid.
3. It was issued NOT due to oxygen shortages but due to concerns the oxygen pipes would not be able to handle the increased flow of oxygen in some hospitals.
At the time, London was the epicentre of Covid. Indeed, elsewhere in the country the demands were considerably lower. There was to my knowledge no threat of oxygen supply problems except for a few hospitals in London. But the directive was national! And many trusts followed it.
It became a new normal across much of the country (including devolved nations) to only admit Covid patients if oxygen levels were 91% or lower. Not 94% as usual, but 91%.
Many ambulance services also changed their 'conveyance' protocols to this new target.
Many ambulance services also changed their 'conveyance' protocols to this new target.
Part of the issue was the wording of the directive.
Note the first part.
The reason for the rationing was concerns about the possible supply/demand issue...
Note the first part.
The reason for the rationing was concerns about the possible supply/demand issue...
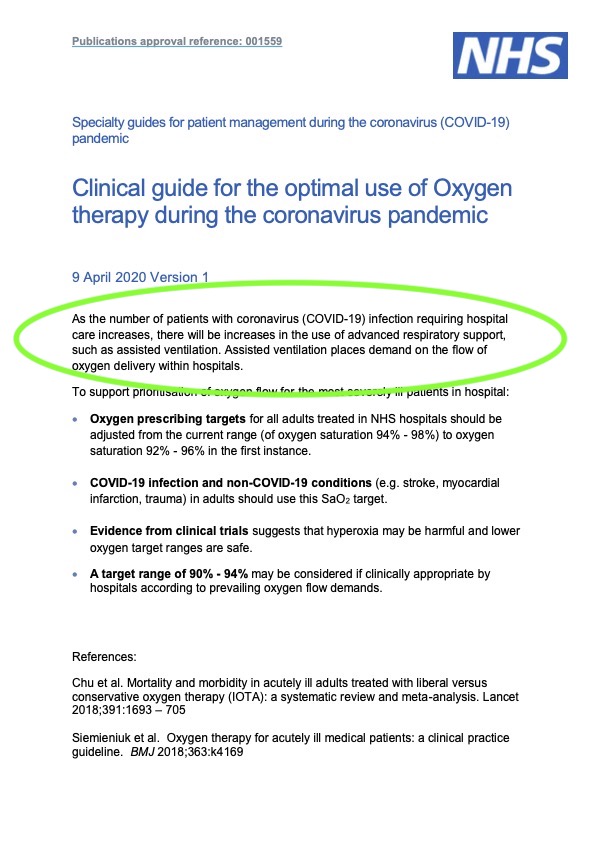
Fine. There isn't enough oxygen so we will need to ration it and until we get more!
But the directive tries to justify the decision as in someway harm-neutral....stating trials suggest 'hyperoxia' (higher than normal) oxygen levels are bad for you and lower levels are safe.
But the directive tries to justify the decision as in someway harm-neutral....stating trials suggest 'hyperoxia' (higher than normal) oxygen levels are bad for you and lower levels are safe.
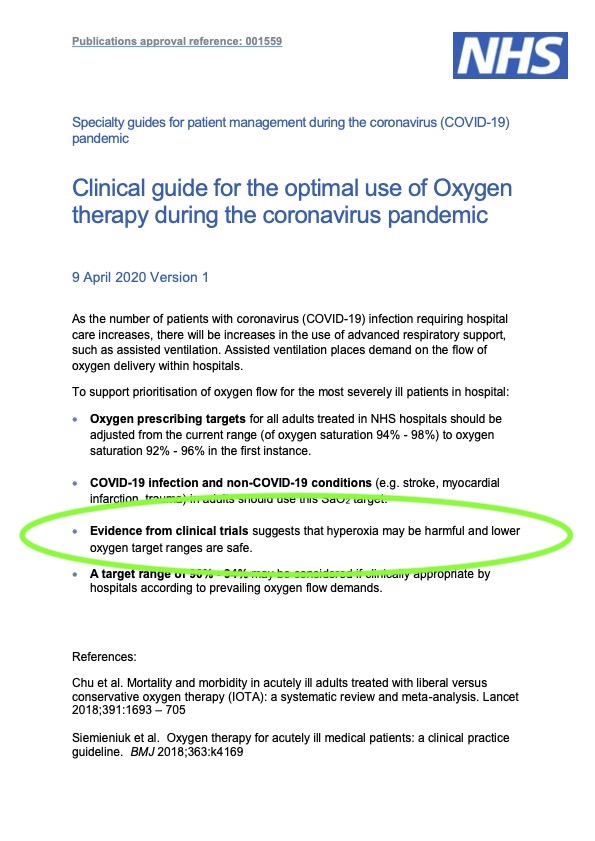
The evidence referenced is the IOTA study of 2018. This study had nothing to do with Covid or pneumonia. The study looked at true hyperoxia, where supernormal levels of oxygen were trialled to 'treat' stroke, heart attack, etc. not hypoxia.
frontiersin.org/articles/10.33…
frontiersin.org/articles/10.33…
NHSE trying to detract from the compromise in care caused by oxygen rationing by suggesting there will be no harm resulting is, IMV, disingenuous and risky.
It has the whiff of 'spin' so typical of our current government...bad news delivered with half truths to lessen the blow.
It has the whiff of 'spin' so typical of our current government...bad news delivered with half truths to lessen the blow.
Rationing oxygen is a sign of failed pandemic controls or pandemic preparedness. Many countries have 'had' to ration oxygen, such as Italy, Brazil and India as they were running out. Other countries did ration oxygen - US, Belgium, Spain - but seemingly not due to supply issues.
The consequences are grave.
There is the issue of sub-optimal/delayed care.
Bigger issue is sending patients home who have clearly progressed to lower lung involvement. They receive no oxygen, often no monitoring, and no supportive treatments such as blood thinners.
There is the issue of sub-optimal/delayed care.
Bigger issue is sending patients home who have clearly progressed to lower lung involvement. They receive no oxygen, often no monitoring, and no supportive treatments such as blood thinners.
So why did the UK, where oxygen was not in short supply, consider it necessary to ration oxygen?
Was the directive motivated by an attempt to reduce hospital admissions?
Where is the evidence of safety for this sudden change in standards?
Was the directive motivated by an attempt to reduce hospital admissions?
Where is the evidence of safety for this sudden change in standards?
Did people come to harm due to this rationing of care?
How many suffered long-term disability due to this policy?
And would quicker action by the UK Gov - flattening the curve earlier - have prevented the concern about oxygen altogether?
Q's for the Covid Inquiry!
How many suffered long-term disability due to this policy?
And would quicker action by the UK Gov - flattening the curve earlier - have prevented the concern about oxygen altogether?
Q's for the Covid Inquiry!
Thankfully, many NHS Trusts have reverted back to our normal British Thoracic Society guidelines for oxygen targets of 94-98%, commencing once oxygen falls below 95%.
But some still believe lower oxygen targets are safe. This, the risk of 'positive spin' in healthcare and science
But some still believe lower oxygen targets are safe. This, the risk of 'positive spin' in healthcare and science
The Bottom Line:
The biggest error was implementing a policy rationing oxygen NATIONALLY.
The second mistake was not to REVERSE it once the wave had passed.
The third was to try and convince clinicians it wasn't a compromise in care.
The biggest error was implementing a policy rationing oxygen NATIONALLY.
The second mistake was not to REVERSE it once the wave had passed.
The third was to try and convince clinicians it wasn't a compromise in care.
At some point the reality of the situation needs to be owned. Yes, care was rationed. Yes, people suffered because of it. Apologies, remediation, and then LEARN.
Another variant looms. A further pandemic is almost certain. A proper Covid Inquiry could be life-saving!
RT pls
Another variant looms. A further pandemic is almost certain. A proper Covid Inquiry could be life-saving!
RT pls
Pandemic Mistakes
Oxygen Rationing
@HeatherHallet10 @CovidJusticeUK @bmj_latest @globalhlthtwit @theAliceRoberts @trishgreenhalgh @dgurdasani1 @chrischirp @Kit_Yates_Maths @HuffPost @GdnHealthcare @ShaunLintern @SusanMichie @microlabdoc @RoryStewartUK @JeremyFarrar
Oxygen Rationing
@HeatherHallet10 @CovidJusticeUK @bmj_latest @globalhlthtwit @theAliceRoberts @trishgreenhalgh @dgurdasani1 @chrischirp @Kit_Yates_Maths @HuffPost @GdnHealthcare @ShaunLintern @SusanMichie @microlabdoc @RoryStewartUK @JeremyFarrar
Pandemic Mistakes
Oxygen Rationing
@MichaelRosenYes @MrNishKumar @MarinaPurkiss @HackedOffHugh @IanMaher7 @Dr2NisreenAlwan @AlisonGeorge10 @AbraarKaran @globalhlthtwit @BinitaKane @PippaCrerar @EricTopol @DrEricDing @mrjamesob @fascinatorfun @drphilhammond @DMinghella
Oxygen Rationing
@MichaelRosenYes @MrNishKumar @MarinaPurkiss @HackedOffHugh @IanMaher7 @Dr2NisreenAlwan @AlisonGeorge10 @AbraarKaran @globalhlthtwit @BinitaKane @PippaCrerar @EricTopol @DrEricDing @mrjamesob @fascinatorfun @drphilhammond @DMinghella
• • •
Missing some Tweet in this thread? You can try to
force a refresh





