*POSTERIORLY DIRECTED MITRAL REGURGITATION*
How many causes of posterior MR do you know?
Let's take a look in this mini 🧵
But...no cheating...vote first!
#echofirst #cardiotwitter #MedTwitter @ASE360 @BSEcho @TheBJCA @BJCA_Women_LTFT @global_wic @WessexSpRs
How many causes of posterior MR do you know?
Let's take a look in this mini 🧵
But...no cheating...vote first!
#echofirst #cardiotwitter #MedTwitter @ASE360 @BSEcho @TheBJCA @BJCA_Women_LTFT @global_wic @WessexSpRs
1. Anterior MV prolapse
Probably the first thing that occurs to most people
AMVL prolapse is less common than PMVL prolapse
Probably the first thing that occurs to most people
AMVL prolapse is less common than PMVL prolapse
Here you can see the highly eccentric, posteriorly directed jet of MR
This is the AP3Ch view showing the same abnormality
2. Systolic Anterior Motion (SAM)
SAM of the AMVL tends to (not always) produce posteriorly directed MR; important to remember that SAM is not the only reason a HCM patient may have MR
PLAX here is not mine, it's from an excellent lecture (on YouTube) by Dr @KyleWKlarich
SAM of the AMVL tends to (not always) produce posteriorly directed MR; important to remember that SAM is not the only reason a HCM patient may have MR
PLAX here is not mine, it's from an excellent lecture (on YouTube) by Dr @KyleWKlarich
Here you can see the posteriorly directed MR jet on colour Doppler imaging
Here is the still image 

3. Ischaemic MR due to posterior leaflet restriction
Inferolateral / inferoposterolateral MI often produces a regional LV abnormality that affects the posteromedial papillary muscle & affects PMVL >> AMVL. The apical PM displacement tethers the PMVL, causing MR
PLAX view here
Inferolateral / inferoposterolateral MI often produces a regional LV abnormality that affects the posteromedial papillary muscle & affects PMVL >> AMVL. The apical PM displacement tethers the PMVL, causing MR
PLAX view here
It may look like there's AMVL prolapse, but if you look closely you'll see the PMVL barely moves
Issue here is PMVL tethering due to inferolateral MI, causing apical displacement of PM pap muscle, thus tethering the leaflet
Issue here is PMVL tethering due to inferolateral MI, causing apical displacement of PM pap muscle, thus tethering the leaflet
As a result, we see this highly eccentric, posteriorly directed MR jet
Here's a still frame of that MR jet
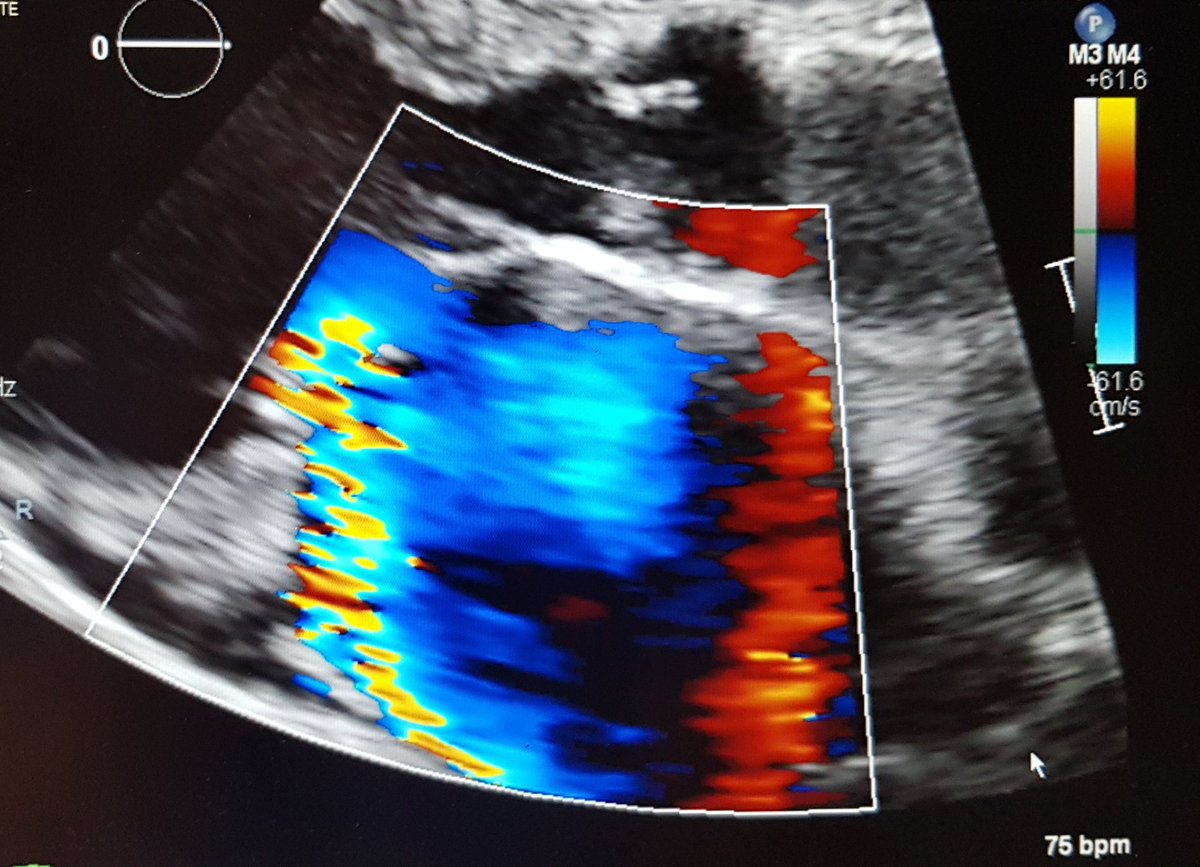
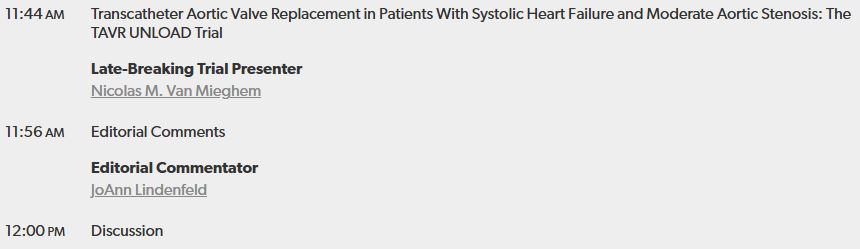
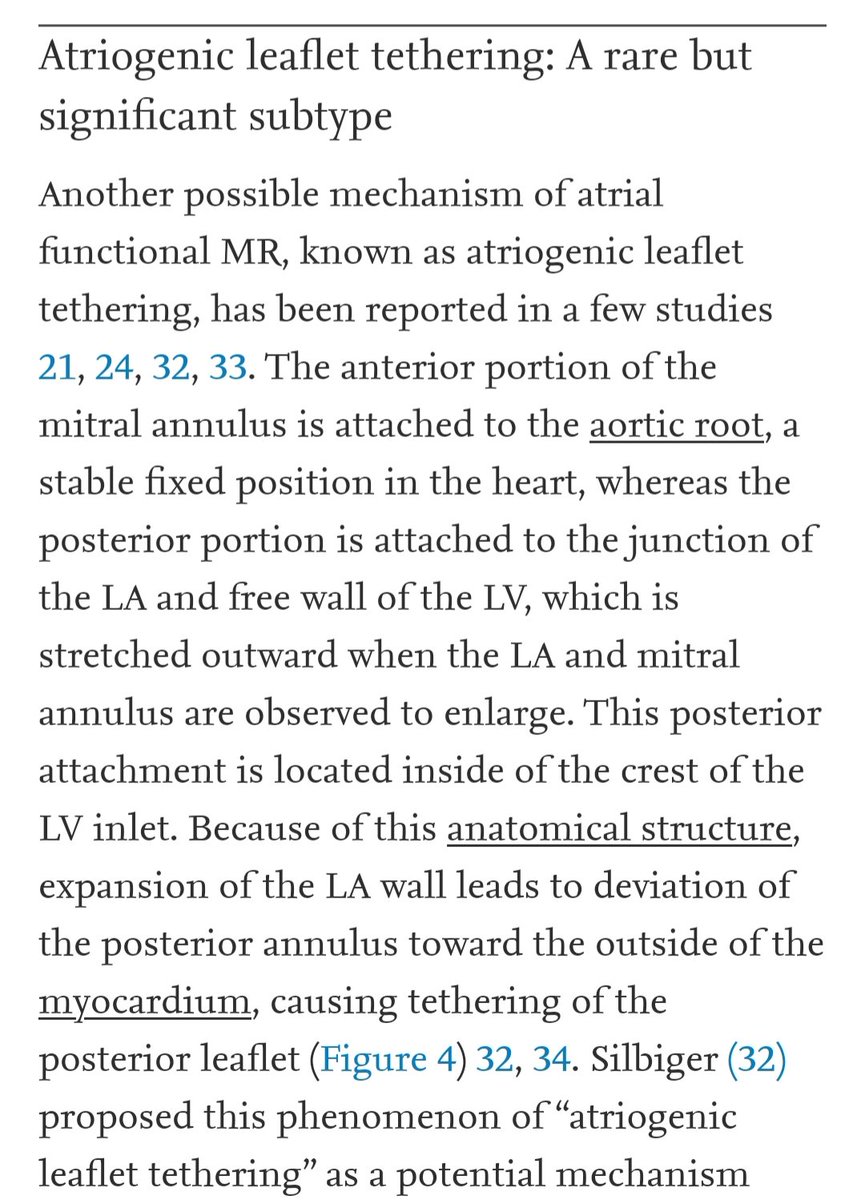
4. Atrial functional MR (AF-MR)
Huge atrial enlargement. There are multiple postulated mechanisms for MR in patients with AF - one is posterior leaflet tethering
Huge atrial enlargement. There are multiple postulated mechanisms for MR in patients with AF - one is posterior leaflet tethering
Again, posteriorly directed MR jet seen here in AP4Ch view
MR still image...
A nice review on AF-MR in JACC Imaging details mechanisms of MR in such patients
@Thind888 @HiteshiKc @suheildhanse @senguptasp @AJamilTajik @renujain19 @BonitaEcho @vonBardelebenRS @doconmoney @SachinGoelMD
@Thind888 @HiteshiKc @suheildhanse @senguptasp @AJamilTajik @renujain19 @BonitaEcho @vonBardelebenRS @doconmoney @SachinGoelMD
These are the 4 main causes of posterior MR that I'm aware of
If you know others, add to the thread! 😁
If you know others, add to the thread! 😁
• • •
Missing some Tweet in this thread? You can try to
force a refresh