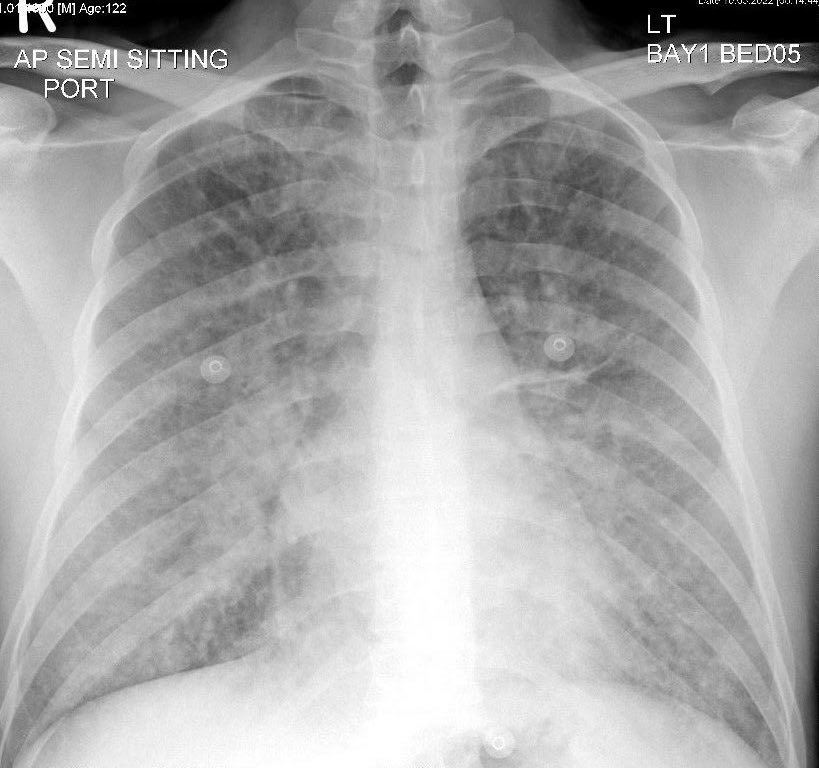
1/n #POCUS case - Pneumothorax. M/20, abrupt left pleuritic chest pain. Absent breath sound left side, hyper-resonant percussion. Absent Pleural sliding on #POCUS . No lung point found, consistent with clinical impression of large pneumothorax.
2/n Normal pleural sliding on #POCUS right anterior thorax
3/n therefore CXR was not a surprise - 

4/n Pneumothorax aspirated with 7 Fr CVC catheter, until resistance to aspiration was felt. #POCUS shows return of pleural sliding and #lungpoint
5/n Appearance of lung point on M-mode - Alternating sea-shore and barcode signs
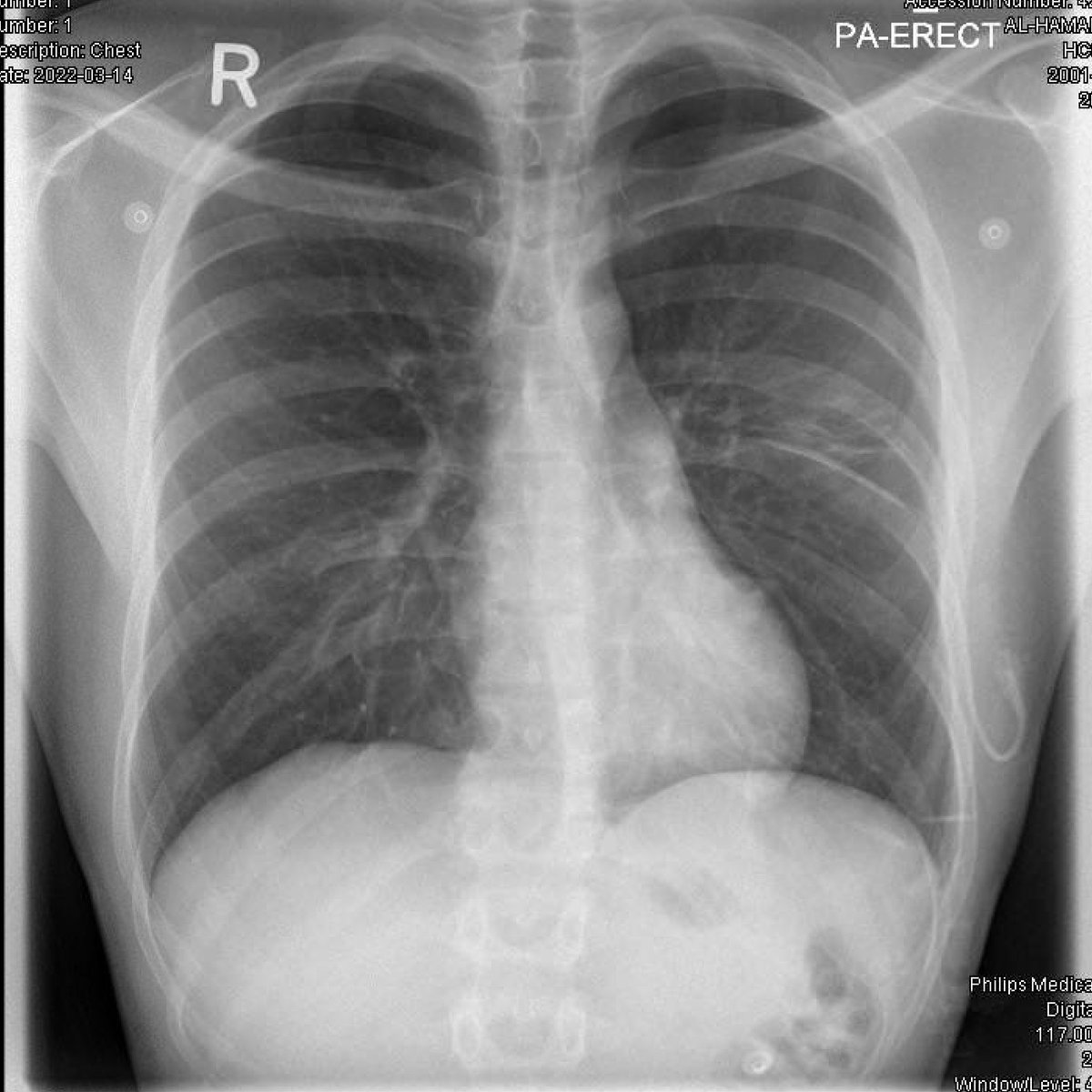
6/6 Observed for 4 hours, repeat #POCUS showed similar findings, CXR repeated, acceptable lung expansion, patient discharged home. ED LOS 5 h.
@threadreaderapp unroll please
• • •
Missing some Tweet in this thread? You can try to
force a refresh