1/ Welcome back to 12-Lead Thursday #MedTwitter !
Let’s get the juices flowing with an EKG! What are the major abnormalities?
Let’s get the juices flowing with an EKG! What are the major abnormalities?

2/ Yes, those are inferolateral ST elevations!
And notice the underlying rhythm of atrial fibrillation
And notice the underlying rhythm of atrial fibrillation

3/ Continuing our patient story, the patient was taken emergently to the cath lab where angiography revealed...
Normal coronary arteries!
Normal coronary arteries!

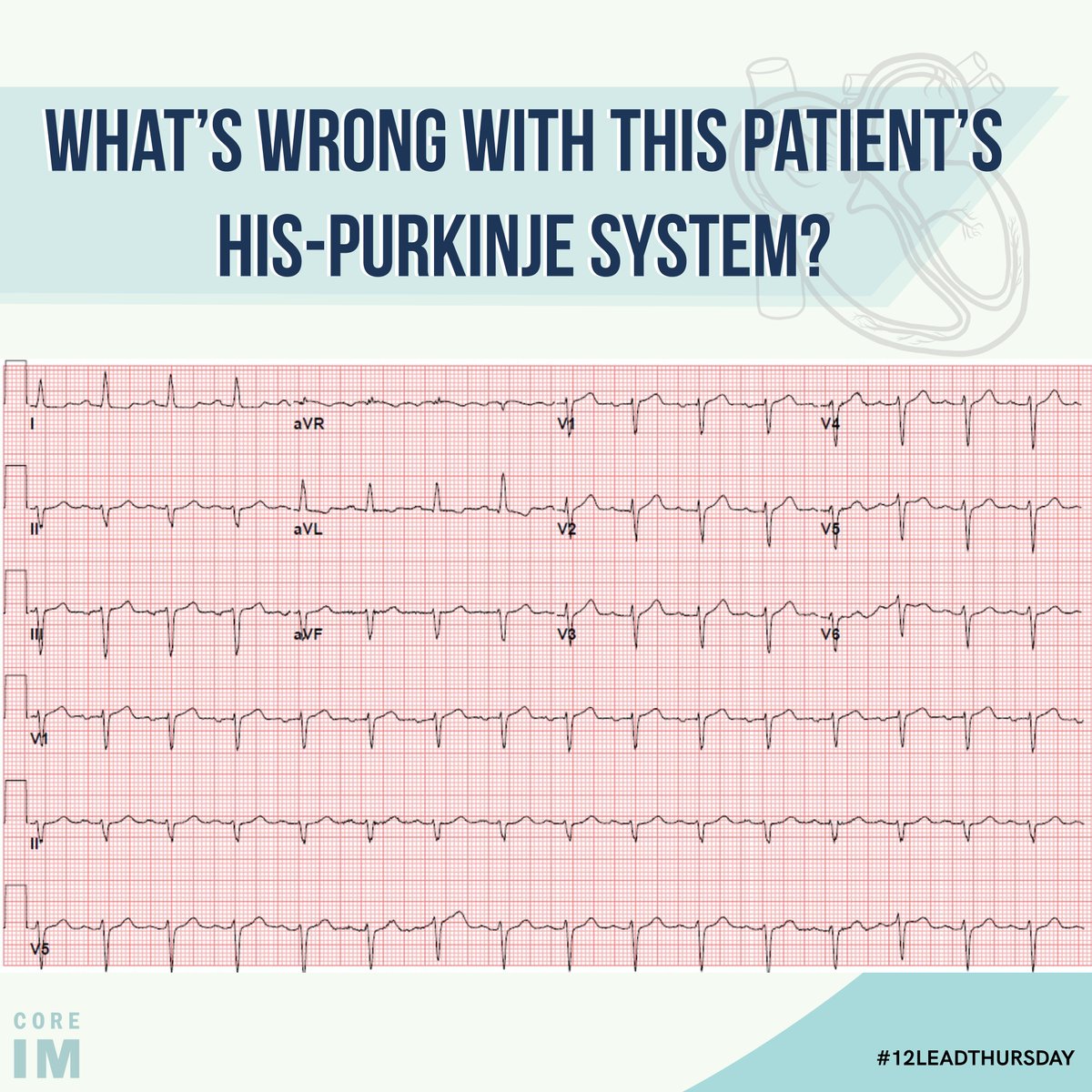
4/ Here is the patient’s EKG from the next day.
Based on the findings in this EKG, what is on your #ddx?
Based on the findings in this EKG, what is on your #ddx?

5/ The deep T waves seen in V4-V6 make us think about:
✅Takotsubo cardiomyopathy
✅Apical variant of hypertrophic cardiomyopathy
✅Ischemia
What is your *most* likely diagnosis at this point?
✅Takotsubo cardiomyopathy
✅Apical variant of hypertrophic cardiomyopathy
✅Ischemia
What is your *most* likely diagnosis at this point?

7/ The progression of these findings clued us in:
☑️ ST elevations on initial presentation
☑️Deep T-wave inversions with QT prolongation
☑️Normalization of EKG
+ the cath to rule out ischemia
It’s Takotsubo cardiomyopathy!
☑️ ST elevations on initial presentation
☑️Deep T-wave inversions with QT prolongation
☑️Normalization of EKG
+ the cath to rule out ischemia
It’s Takotsubo cardiomyopathy!

8/ And while the EKG is helpful for Takotsubo, more is needed for the diagnosis:
- transient wall motion abnormalities (apical ballooning and akinesis)
- absence of obstructive coronary disease
- new EKG abnormalities
-absence of pheochromocytoma and myocarditis
- transient wall motion abnormalities (apical ballooning and akinesis)
- absence of obstructive coronary disease
- new EKG abnormalities
-absence of pheochromocytoma and myocarditis

9/ Thanks for tuning into this week’s #12LeadThursday. This byte was authored by Dena Hayes MD with edits by Sam Maidman MD and @gregorykatz . Graphics by Ivanna Tang.
See you next time!
See you next time!
• • •
Missing some Tweet in this thread? You can try to
force a refresh