
The largest trial of #ivermectin in early #COVID is now published @NEJM & the results are *NEGATIVE*
#TOGETHER randomized n=1358 outpatients with COVID in 🇧🇷 to IVM vs placebo. No difference in hospitalizations, mechanical ventilation, or death.
nejm.org/doi/full/10.10…
A 🧵
1/
#TOGETHER randomized n=1358 outpatients with COVID in 🇧🇷 to IVM vs placebo. No difference in hospitalizations, mechanical ventilation, or death.
nejm.org/doi/full/10.10…
A 🧵
1/



I’ve written about the #TOGETHER trial before (see my fluvoxamine 🧵below)
Briefly #TOGETHER is a large double blind multi-arm platform RCT. Pretty much the 1st 🥇 gold standard for high quality medical research.
2/
Briefly #TOGETHER is a large double blind multi-arm platform RCT. Pretty much the 1st 🥇 gold standard for high quality medical research.
2/
https://twitter.com/nickmmark/status/1453500711266766849
TOGETHER enrolled high risk people with COVID from 12 outpatient clinics in Brazil.
Patients could be enrolled up to 7 days after symptom onset (more on this later).
They were randomized to either placebo or to ivermectin 0.4mg/kg daily for 3 days. (Also more on dose later)
3/
Patients could be enrolled up to 7 days after symptom onset (more on this later).
They were randomized to either placebo or to ivermectin 0.4mg/kg daily for 3 days. (Also more on dose later)
3/


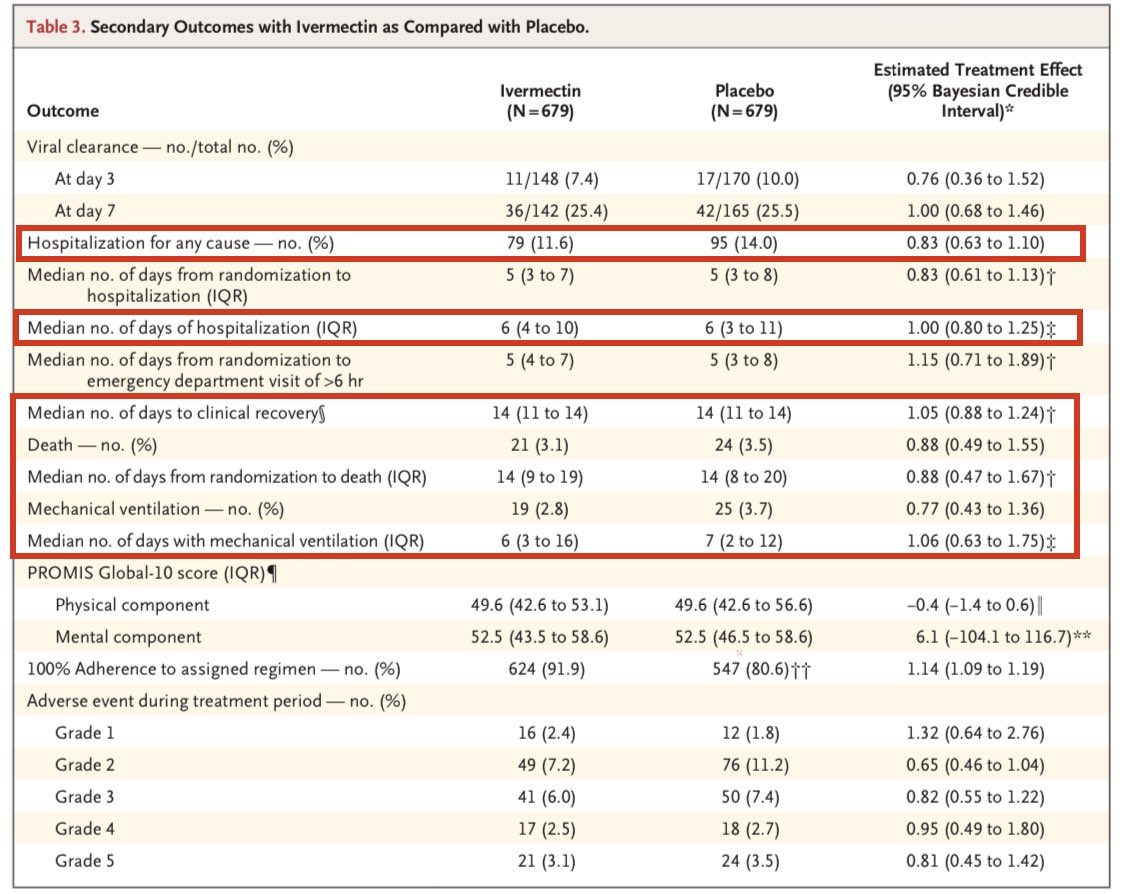
The primary endpoint was a composite of hospitalization or >6hr ED visit. (Not an awesome primary endpoint IMO 🤷).
Secondary endpoints included: time until hospitalization, hospital LOS, need for mechanical ventilation, duration of MV, and death. (All very reasonable 👍)
4/
Secondary endpoints included: time until hospitalization, hospital LOS, need for mechanical ventilation, duration of MV, and death. (All very reasonable 👍)
4/
It enrolled n=1358 people.
The patients were slightly younger (median age 49) with the expected mix of comorbid conditions seen in COVID (DM2, HTN, asthma).
The groups appear well balanced (see my prior thread about the likely fraudulent vitamin C paper for more on this.)
5/
The patients were slightly younger (median age 49) with the expected mix of comorbid conditions seen in COVID (DM2, HTN, asthma).
The groups appear well balanced (see my prior thread about the likely fraudulent vitamin C paper for more on this.)
5/

The study was stone cold NEGATIVE.
There was NO statistically significant difference in the primary endpoint or *ANY* of the secondary endpoints.
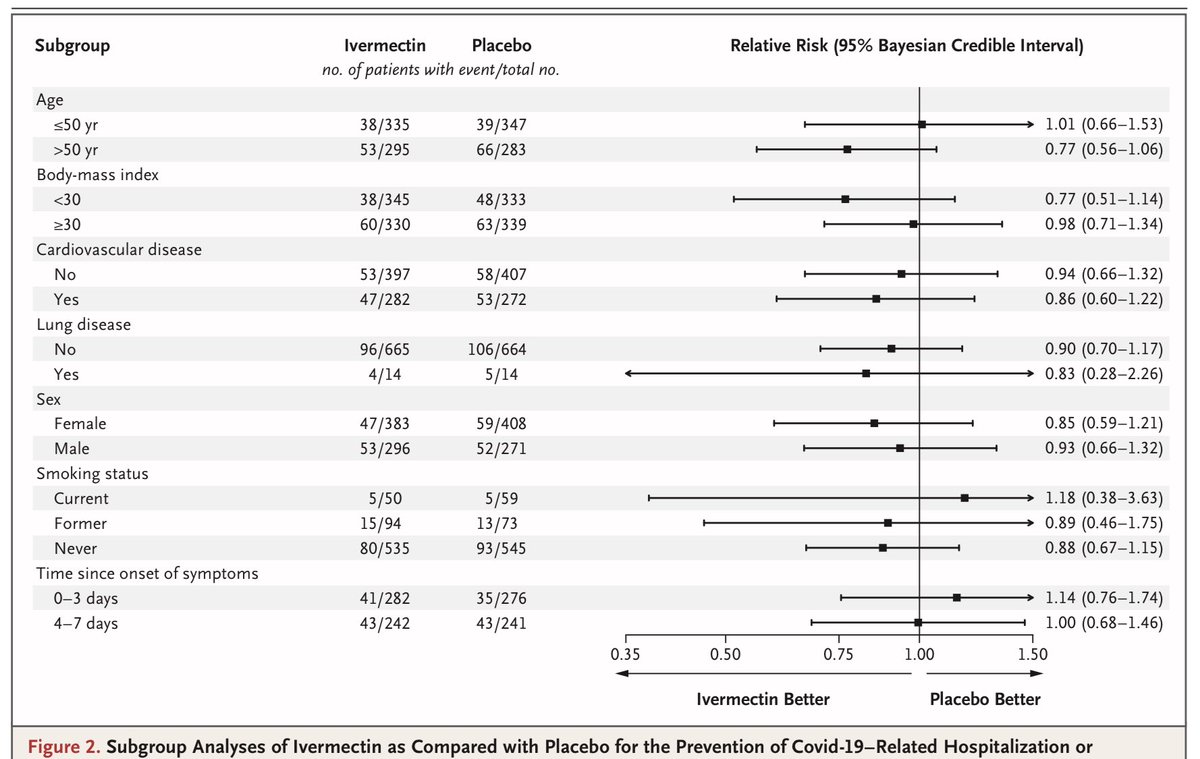
Beyond the overall negative findings, there was no prespecified subgroup that benefited from ivermectin.
Super duper negative.
6/
There was NO statistically significant difference in the primary endpoint or *ANY* of the secondary endpoints.
Beyond the overall negative findings, there was no prespecified subgroup that benefited from ivermectin.
Super duper negative.
6/



Now let’s address some of the likely #CultOfIvermectin criticisms:
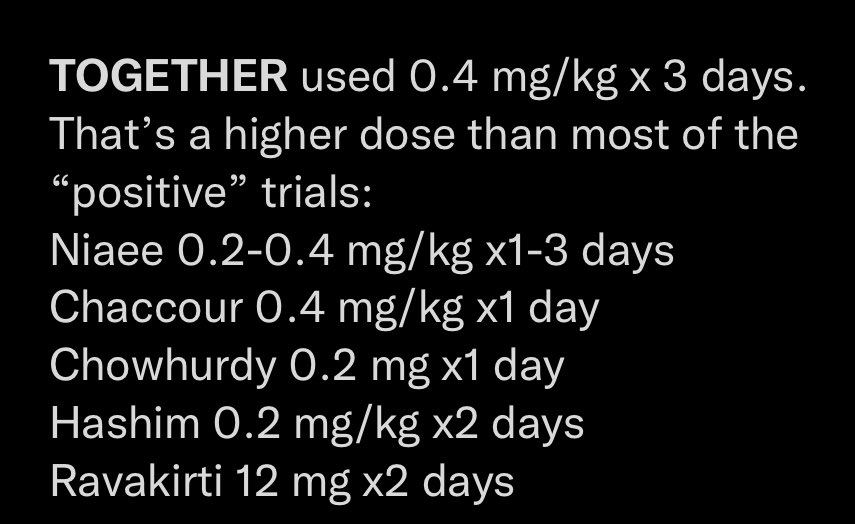
“BuT tHe IvErMeCtIn dOsE wAs ToOoO LoW!”
#TOGETHER used a dose twice as high as the FDA approved dose of ivermectin: 0.2mg/kg
#TOGETHER also used a higher dose than most of the low quality “positive” trials.
7/
“BuT tHe IvErMeCtIn dOsE wAs ToOoO LoW!”
#TOGETHER used a dose twice as high as the FDA approved dose of ivermectin: 0.2mg/kg
#TOGETHER also used a higher dose than most of the low quality “positive” trials.
7/
https://twitter.com/nickmmark/status/1454252241381040132
“BuT tReAtMeNt sTaRtEd ToOoOo LaTe!”
Roughly half the patients (44%) got treatment within 3 days. That’s early. Among the patients who were treated earlier they did… worse!
8/
Roughly half the patients (44%) got treatment within 3 days. That’s early. Among the patients who were treated earlier they did… worse!
8/


Also if we look at the patients who *completed* the 3 day course of ivermectin (per-protocol analysis) they actually did *worse* than the intention to treat group.
If ivermectin really worked, you might expect the people who completed a course of it to better. They didn’t.
9/
If ivermectin really worked, you might expect the people who completed a course of it to better. They didn’t.
9/

“BuT mOrTaLiTy wAs LoWeR!”
A common misconception about stats.
Let’s look at the 0.88 mortality effect.
The confidence intervals mean there is a 95% chance that mortality is between 51% less OR 55% more with IVM.
Would *YOU* take a drug that might increase mortality by 55%?
10/
A common misconception about stats.
Let’s look at the 0.88 mortality effect.
The confidence intervals mean there is a 95% chance that mortality is between 51% less OR 55% more with IVM.
Would *YOU* take a drug that might increase mortality by 55%?
10/


“tHe tRiAl WaS dEsIgNeD tO fAiL bY eViL pHaRmA!”
This was one arm of a *multi-arm study*. Another arm of #TOGETHER found that a repurposed cheap generic med (fluvoxamine) *improved* outcomes in COVID.
How (& why) would an evil cabal sabotage just one arm of a multi arm RCT?
11/
This was one arm of a *multi-arm study*. Another arm of #TOGETHER found that a repurposed cheap generic med (fluvoxamine) *improved* outcomes in COVID.
How (& why) would an evil cabal sabotage just one arm of a multi arm RCT?
11/
Related dumb criticism:
“ThE vAcCiNeS wOuLd LoSe tHiEr EUA iF iVeRmEcTiN wAs PrOvEn!”
This is nonsense. The EUA for *vaccines* to prevent severe disease has nothing to do with the absence of therapies. Otherwise Dex, Bari, Toci, etc would have already “voided the EUAs”
12/
“ThE vAcCiNeS wOuLd LoSe tHiEr EUA iF iVeRmEcTiN wAs PrOvEn!”
This is nonsense. The EUA for *vaccines* to prevent severe disease has nothing to do with the absence of therapies. Otherwise Dex, Bari, Toci, etc would have already “voided the EUAs”
12/
“ThIs iS jUsT oNe StUdY!”
This is the largest RCT to date.
👉Every single large RCT has found no survival benefit to ivermectin in COVID. Every one. For example:
#EPIC bit.ly/370lgSi
#IVERCORCOVID bit.ly/3DrkMRx
#ITECH bit.ly/3wMBbyF
13/
This is the largest RCT to date.
👉Every single large RCT has found no survival benefit to ivermectin in COVID. Every one. For example:
#EPIC bit.ly/370lgSi
#IVERCORCOVID bit.ly/3DrkMRx
#ITECH bit.ly/3wMBbyF
13/



On the other hand the *only* trials that have found *any* benefit to ivermectin are:
- fraudulent (Surgisphere, Elegazzar, etc)
- flawed observational studies that are likely biased
- tiny studies looking at non patient centered outcomes like viral load
14/
- fraudulent (Surgisphere, Elegazzar, etc)
- flawed observational studies that are likely biased
- tiny studies looking at non patient centered outcomes like viral load
14/
https://twitter.com/nickmmark/status/1446519197387821057
Clinical 🥡 points:
#TOGETHER is the largest RCT of ivermectin to date. It found that early high dose ivermectin did NOT prevent hospitalization, mechanical ventilation, or mortality in high risk outpatients with COVID.
All prior (non-fraudulent RCTs) have found the same.
15/
#TOGETHER is the largest RCT of ivermectin to date. It found that early high dose ivermectin did NOT prevent hospitalization, mechanical ventilation, or mortality in high risk outpatients with COVID.
All prior (non-fraudulent RCTs) have found the same.
15/
You can read more about this here: onepagericu.com/blog/debunking…
You can also watch a grand rounds I did at @NJHealth debunking ivermectin:
16/
You can also watch a grand rounds I did at @NJHealth debunking ivermectin:
16/
• • •
Missing some Tweet in this thread? You can try to
force a refresh































