The #CultOfIvermectin has invented new excuses. Let’s address those:
“eVeRyOnE iN bRaZiL wAs AlReAdY TaKiNg IvErMeCtIn OTC!”
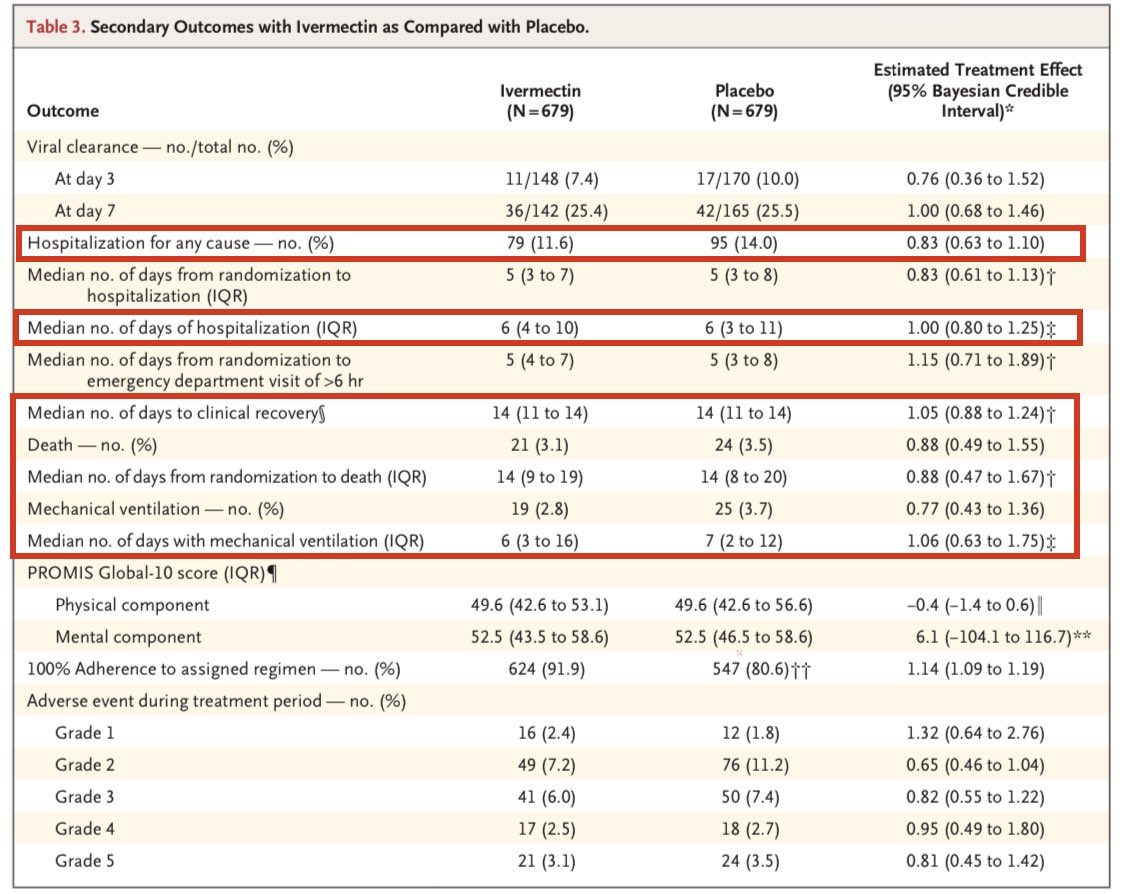
While Ivermectin use in the 30 days prior to screening wasn’t an absolute exclusion criteria, they appear to have de facto excluded those patients.
1/
“eVeRyOnE iN bRaZiL wAs AlReAdY TaKiNg IvErMeCtIn OTC!”
While Ivermectin use in the 30 days prior to screening wasn’t an absolute exclusion criteria, they appear to have de facto excluded those patients.
1/
https://twitter.com/nickmmark/status/1509295028673269761


It’s also worth wondering *why* someone who was taking ivermectin would enroll in a RCT of ivermectin vs placebo.
Also - if ivermectin prophylaxis was so effective - why would so many people on ivermectin be getting COVID in the first place?
2/
Also - if ivermectin prophylaxis was so effective - why would so many people on ivermectin be getting COVID in the first place?
2/
“tHeY dIdN’t UsE ZINC!!!!”
The original in vitro studies of ivermectin (Caly et al) didn’t use zinc.
None of the fraudulent “positive” RCTs of ivermectin combined it with zinc.
There has been *one* RCT of early zinc in COVID and it was *NEGATIVE*.
jamanetwork.com/journals/jaman…
3/
The original in vitro studies of ivermectin (Caly et al) didn’t use zinc.
None of the fraudulent “positive” RCTs of ivermectin combined it with zinc.
There has been *one* RCT of early zinc in COVID and it was *NEGATIVE*.
jamanetwork.com/journals/jaman…
3/
Claiming that a highly effective “treatment protocol” is a combination of therapies that are individually useless is bizarre.
Continuously adding more meds to the protocol is really just moving the goal posts. Every time a new RCT is negative they claim it didn’t include “x.”
4/
Continuously adding more meds to the protocol is really just moving the goal posts. Every time a new RCT is negative they claim it didn’t include “x.”
4/
It takes time to do a RCT.
FLCCC updated their “protocols” dozens of times to stay ahead of the negative studies.
Recently they added hydroxychloroquine - another disproven therapy. No doubt they will next claim that IVM & HCQ are both necessary to “miraculously cure COVID.”
5/
FLCCC updated their “protocols” dozens of times to stay ahead of the negative studies.
Recently they added hydroxychloroquine - another disproven therapy. No doubt they will next claim that IVM & HCQ are both necessary to “miraculously cure COVID.”
5/

• • •
Missing some Tweet in this thread? You can try to
force a refresh