Q: What do🐍 snakes have to do with ICU pharmacology?
A: A lot! We use 💊medications derived from snake venom every day in fact!
Buckle up for a fun 🧵of #UnusualDrugDiscovery & #HistoryOfMedicine about medications derived from from 🐍☠️snake venom! #FOAMed #FridayFun
1/
A: A lot! We use 💊medications derived from snake venom every day in fact!
Buckle up for a fun 🧵of #UnusualDrugDiscovery & #HistoryOfMedicine about medications derived from from 🐍☠️snake venom! #FOAMed #FridayFun
1/




First a question: which of the following snake venoms have been used to develop medical therapies?
(don't worry we’ll go over the answer at the end)
2/
(don't worry we’ll go over the answer at the end)
2/
It was long known that workers in banana plantations would collapse due to low blood pressure if they were bitten by the Brazilian Arrow Headed Pit Viper Bothrops jararaca.
A Brazilian graduate student - Sergio Ferreira - thought this could be useful...
3/
A Brazilian graduate student - Sergio Ferreira - thought this could be useful...
3/


Analyzing Bothrops jararaca venom, Ferreira identified a peptide that inhibited ACE. He called it bradykinin potentiating peptide (BPP).
A decade of hard work later, chemists turned that peptide into an orally available small molecule: CAPTOPRIL (the first ACE inhibitor).
4/
A decade of hard work later, chemists turned that peptide into an orally available small molecule: CAPTOPRIL (the first ACE inhibitor).
4/



Next time you prescribe a “__OPRIL" remember the 1st ACEI (& template for the entire class) was Brazilian Viper derived.
Fun Fact: in the 1980s they leaned into this fact hard, including having cardiology conference attendees visit a snake farm!
pharmaceutical-journal.com/article/news/f…
5/
Fun Fact: in the 1980s they leaned into this fact hard, including having cardiology conference attendees visit a snake farm!
pharmaceutical-journal.com/article/news/f…
5/
The bite of some snakes can cause significant hemorrhage.
Occasionally the victim will even bleed spontaneously at sites remotely from where they were bitten.
Why?
6/
Occasionally the victim will even bleed spontaneously at sites remotely from where they were bitten.
Why?
6/
It turns out that some snake venoms contain glycoprotein IIb/IIIa inhibitors!
For example:
The pygmy rattlesnake (Sistrurus miliarius) in the southern US (left), & the saw-scaled viper (Echis spp) in Africa, India, & the Middle East (right).
7/
For example:
The pygmy rattlesnake (Sistrurus miliarius) in the southern US (left), & the saw-scaled viper (Echis spp) in Africa, India, & the Middle East (right).
7/
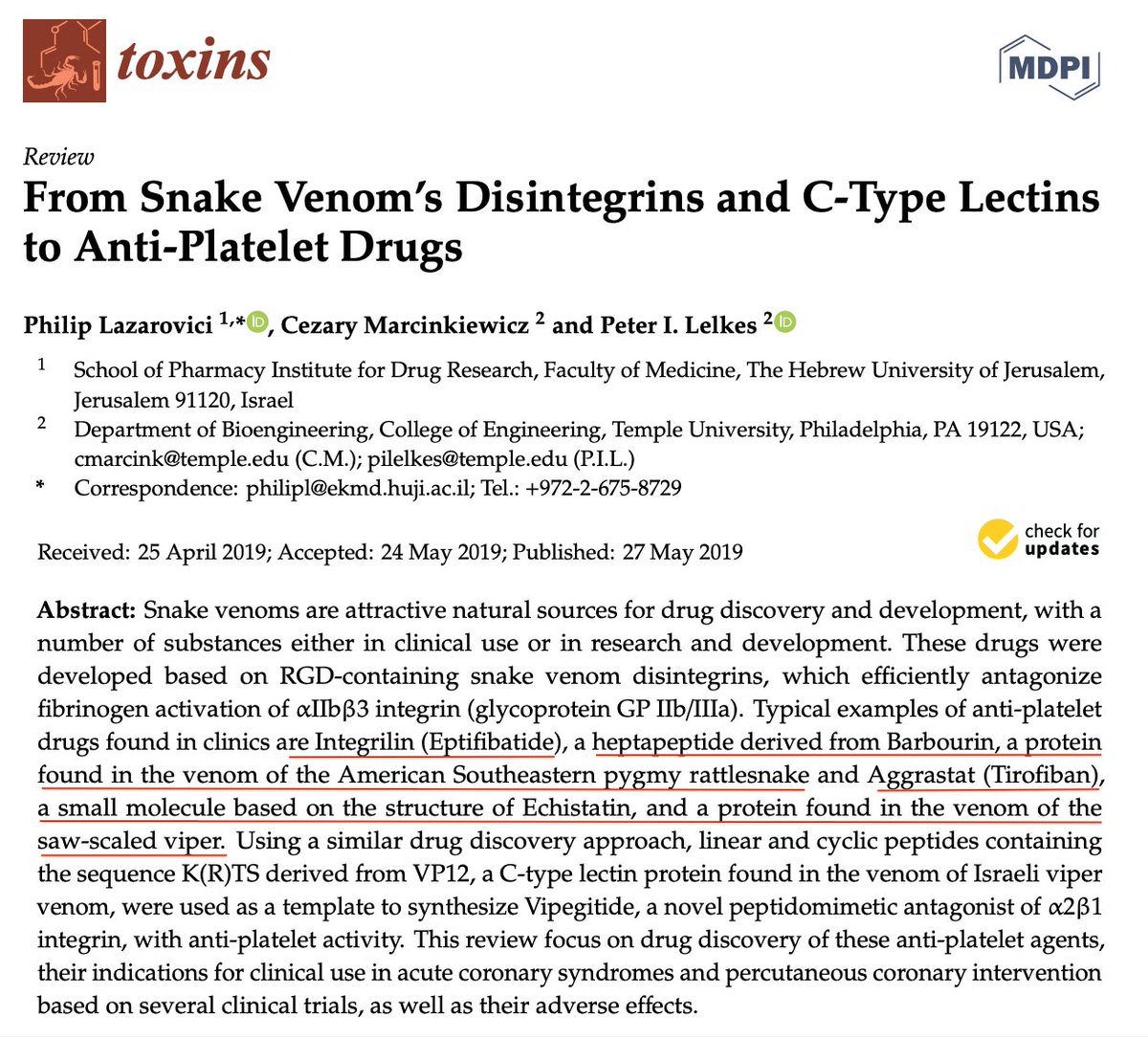



In fact this is where not one, but TWO clinically useful anti-platelet medications come from:
pygmy rattlesnake (Sistrurus miliarius) —> eptifibatide
saw-scaled viper (Echis spp) —> tirofibran
ncbi.nlm.nih.gov/pmc/articles/P…
How many people having ACS have been saved by snake venom?
8/
pygmy rattlesnake (Sistrurus miliarius) —> eptifibatide
saw-scaled viper (Echis spp) —> tirofibran
ncbi.nlm.nih.gov/pmc/articles/P…
How many people having ACS have been saved by snake venom?
8/
Not all snake venoms make you bleed; some make you clot.
This observation was actually used clinically in the 1930s to control hemorrhage in people w/ hemophilia.
I *highly* recommend reading this article about it:
onlinelibrary.wiley.com/doi/10.1111/j.…
9/
This observation was actually used clinically in the 1930s to control hemorrhage in people w/ hemophilia.
I *highly* recommend reading this article about it:
onlinelibrary.wiley.com/doi/10.1111/j.…
9/



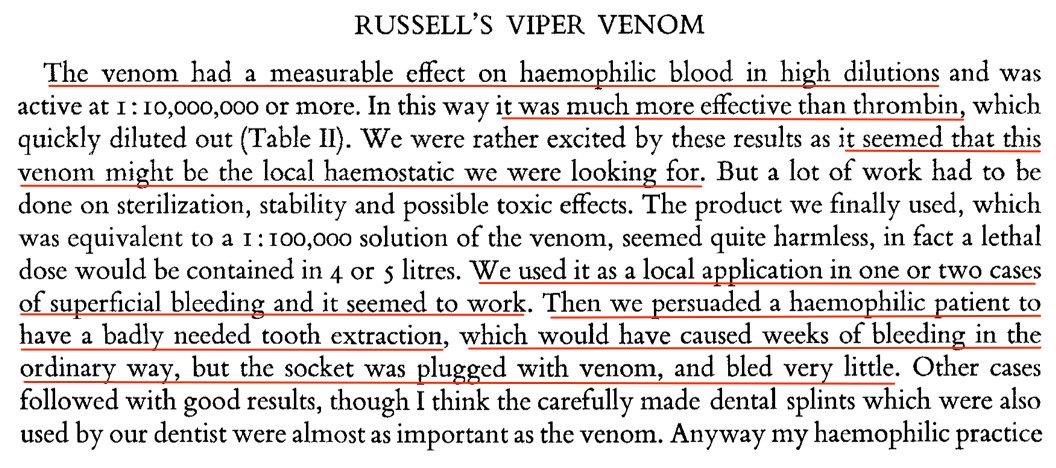
This research found that one snake in particular - Russell's viper (Daboia russelii) - causes very fast clotting!
It clotted blood from hemophiliacs in just seconds!
10/
It clotted blood from hemophiliacs in just seconds!
10/

Since the invention of factor replacement, we don’t use Russel’s viper venom (RVV) to stop bleeding anymore.
But RVV is still used every day to stimulate clotting in vitro and to detect the presence of lupus anticoagulant.
11/
But RVV is still used every day to stimulate clotting in vitro and to detect the presence of lupus anticoagulant.
11/


👀 You can even order a Russell viper venom test in EPIC! Next time you are testing for Lupus Anticoagulant, remember the Snake that makes its detection possible.
(Also think about the unlucky person who has to extract the venom that makes the dRVVV test possible!)
12/
(Also think about the unlucky person who has to extract the venom that makes the dRVVV test possible!)
12/


Bonus case: 🦎 The Gila Monster (Heloderma suspectum) aka the “most venomous lizard in the world” with “the most painful venom of any vertebrate”
Yikes!
(yes I know this isn't a snake but it's too interesting for us *not* to discuss it!)
13/
Yikes!
(yes I know this isn't a snake but it's too interesting for us *not* to discuss it!)
13/



Fortunately while the Gila monster may be “the most venomous lizard in the world” and “has the most painful venom" it’s also just about the slowest moving lizard ever.
As this pioneering Arizona Doc put it:
14/
As this pioneering Arizona Doc put it:
14/

While Gila monster bites are rare, there are cases. Including one guy who "purposely provoked one of his captive lizard into biting him on his finger."
One observation of people bitten by Gila monsters is that they sometimes developed hypoglycemia afterwards.
15/
One observation of people bitten by Gila monsters is that they sometimes developed hypoglycemia afterwards.
15/

This led researchers to suspect there was something in the venom effecting insulin.
In the 1980s & 1990s, an insulin secretologue was identified in Gila monster venom.
This led to a synthetic derivative: exenatide which was FDA approved for in 2005. One of the newest DM meds!
16/
In the 1980s & 1990s, an insulin secretologue was identified in Gila monster venom.
This led to a synthetic derivative: exenatide which was FDA approved for in 2005. One of the newest DM meds!
16/


Summary:
At least 4 different snakes 🐍 (& the Gila monster 🦎) have contributed to drug development with their venom.
The products of snake venom include: ACE inhibitors, GPIIb/IIIa inhibitors, GLP-1 agonists, & the test for Lupus Anticoagulant.
#UnusualDrugDiscovery
17/
At least 4 different snakes 🐍 (& the Gila monster 🦎) have contributed to drug development with their venom.
The products of snake venom include: ACE inhibitors, GPIIb/IIIa inhibitors, GLP-1 agonists, & the test for Lupus Anticoagulant.
#UnusualDrugDiscovery
17/

• • •
Missing some Tweet in this thread? You can try to
force a refresh