Am I taking a break from pandemic-related news? Is the pandemic over? No, then why in the midst of the pandemic, I’m doing this long thread on something different? Will disclose the reason in the end.....but I think this fascinating tale needed to be told to my twitter family 1/
Most of my close associates are aware of this saga. But most of the Twitterati are oblivious of this journey. It all started in the autumn of 1998 when I got two young kids with a weird behaviour—combative & agitated, chewing their body parts along w/ fever, vomiting, stupor.. 2/ 


Clinically and even after performing basic investigations, their clinical profile was not fitting in a proper known clinical entity. It was not encephalitis, not hepatic coma, nor another known multi-system disease. And this was not a stray incident. 3/
For next two months, I treated 6 such cases. Unfortunately, most died within few hours to a couple of days of admission. And the same pattern was repeated for next 8-9 years! Frankly speaking, I had never witnessed such cases. 4/

There was severe hypoglycaemia, markedly raised liver/ muscle enzymes, normal CSF & CNS imaging. Most succumbing within 24-48 hours with a very high mortality (75%). Few rare cases who survived had rapid improvement without any psycho-neurological deficit. 5/
Presumptively, I labelled them as cases Reye-like encephalopathy, and published these findings in a peer-reviewed journal. 6/
pubmed.ncbi.nlm.nih.gov/10750089/
pubmed.ncbi.nlm.nih.gov/10750089/

At this time, I realized that the disease was not confined to my district (Bijnor) alone. During the past 2 decades, annually during autumn months, young children died in large numbers in many districts of western UP, Uttarakhand, & Haryana with a peculiar disease. 7/

#Saharanpur was the epicentre; hence the entity was referred as “Saharanpur Encephalitis”! Around 500-700 children affected annually, >80% dying! Most deaths went un-reported, un-diagnosed!! I wrote few pieces in @EditorIndPed in this regard 8/
pubmed.ncbi.nlm.nih.gov/14530570/
pubmed.ncbi.nlm.nih.gov/14530570/



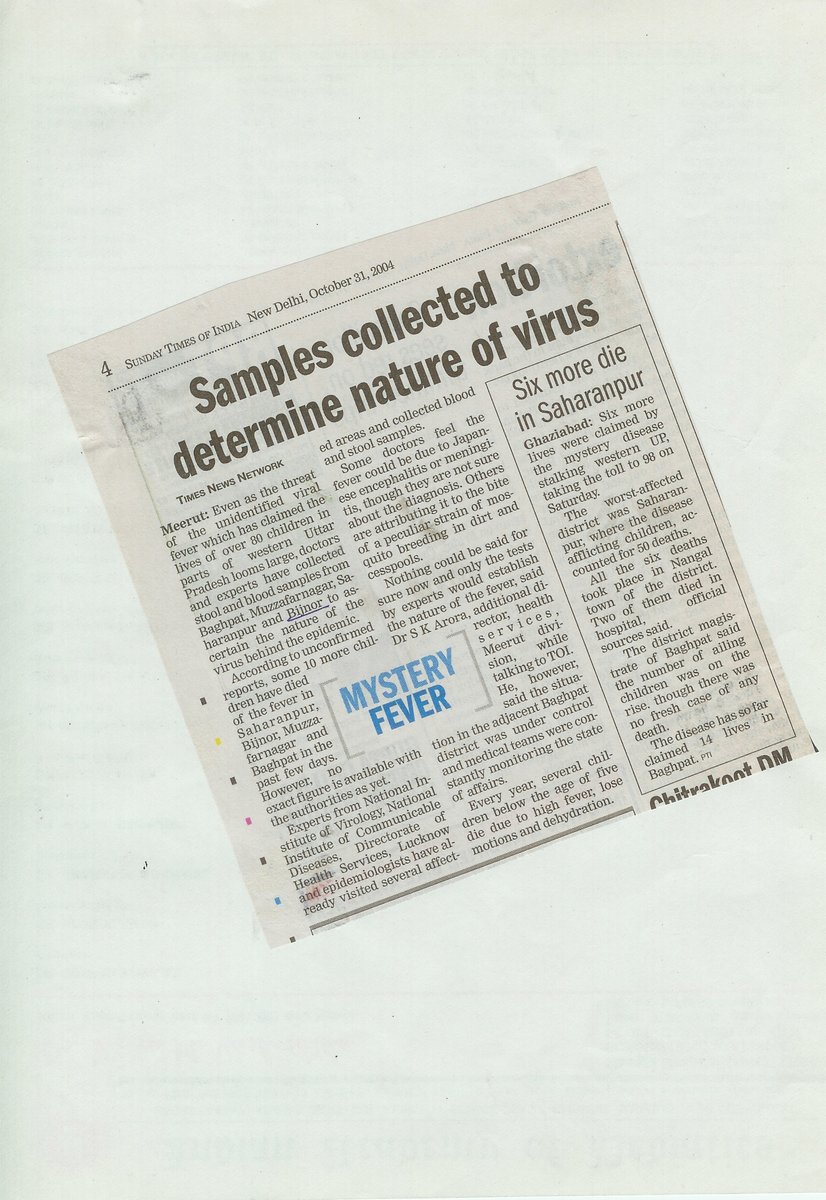
Local media was the first & the only source of having some info about these cases. Not only the academicians/agencies were confused, but there was confusion all around!! Look for the headline “Cool weather….”. 9/



One academic paper describes the illness, “The seasonal distribution favors Reye’s syndrome, the clinical presentation favor Nipah virus, the epidemiological factors points to JE or some other viral illness with a common source.” 10/
indianpediatrics.net/apr2007/apr-31…
indianpediatrics.net/apr2007/apr-31…

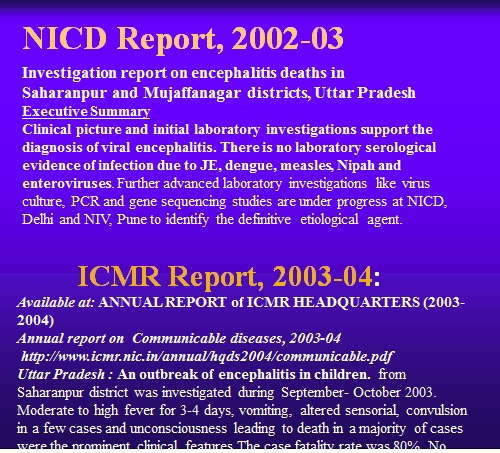
Even the @WHO, @ICMRDELHI & @Director_NCDC teams were suspecting acute viral encephalitis caused by an unknown virus that remains active during early winter months (Sept-Dec). 11/


During next couple of years, I approached different investigating agencies, particularly NICD (now NCDC). In 2003, I decided to seek help from other non-Govt experts & forge a team. At this time, I approached Dr T Jacob John who was deeply interested in these outbreaks. 12/
#TJacobJohn also wrote a viewpoint article citing the western UP ongoing outbreaks. He cited my personal interaction on this particular outbreak & stressed the need to differentiate encephalitis from encephalopathy! 13/
pubmed.ncbi.nlm.nih.gov/14530546/
pubmed.ncbi.nlm.nih.gov/14530546/

He wrote, “it is important to educate....on such outbreaks & help Public Health officials to refrain from bringing bad name to India by declaring that this disease has mysterious origin, a concept discarded by Ayurveda in ancient times & by science in modern times” 14/
At this time, I decided to start further investigations in collaboration with #TJacobJohn who was based in Vellore, since the Govt agencies were reluctant to collaborate with a private doctor. So, it was the first step in the formation of a team.. 15/
Next logical step was to further investigate these cases. On TJJ’s advice, I performed 21 liver biopsies (including 5 postmortem tissues), brain biopsies (in two cases) and several tibial muscle biopsies of these poor children based on the clinical pointers. 16/
I sent few liver specimens/slides to several reputed labs including some of the most renowned national chains, but most either reported normal tissue or acute viral hepatitis. But it was not supporting our clinical impression: a case of Reye-like syndrome! 17/
Later, I googled & reviewed literature, and found a retired professor of AIIMS, New Delhi who had done a lot of work in childhood Cirrhosis, fatty liver & hepatic carcinoma. His name was Nabeen C Nayak. He became the third member of our team. 18/
I forwarded some liver tissue to him at @GangaRamHospit1 where he was affiliated at that time. On going through few slides, he jumped on his seat & called me: 'Vipin, we are dealing with a ‘toxin-mediated’ necrosis of liver". Reye-syndrome was ruled out! 19/


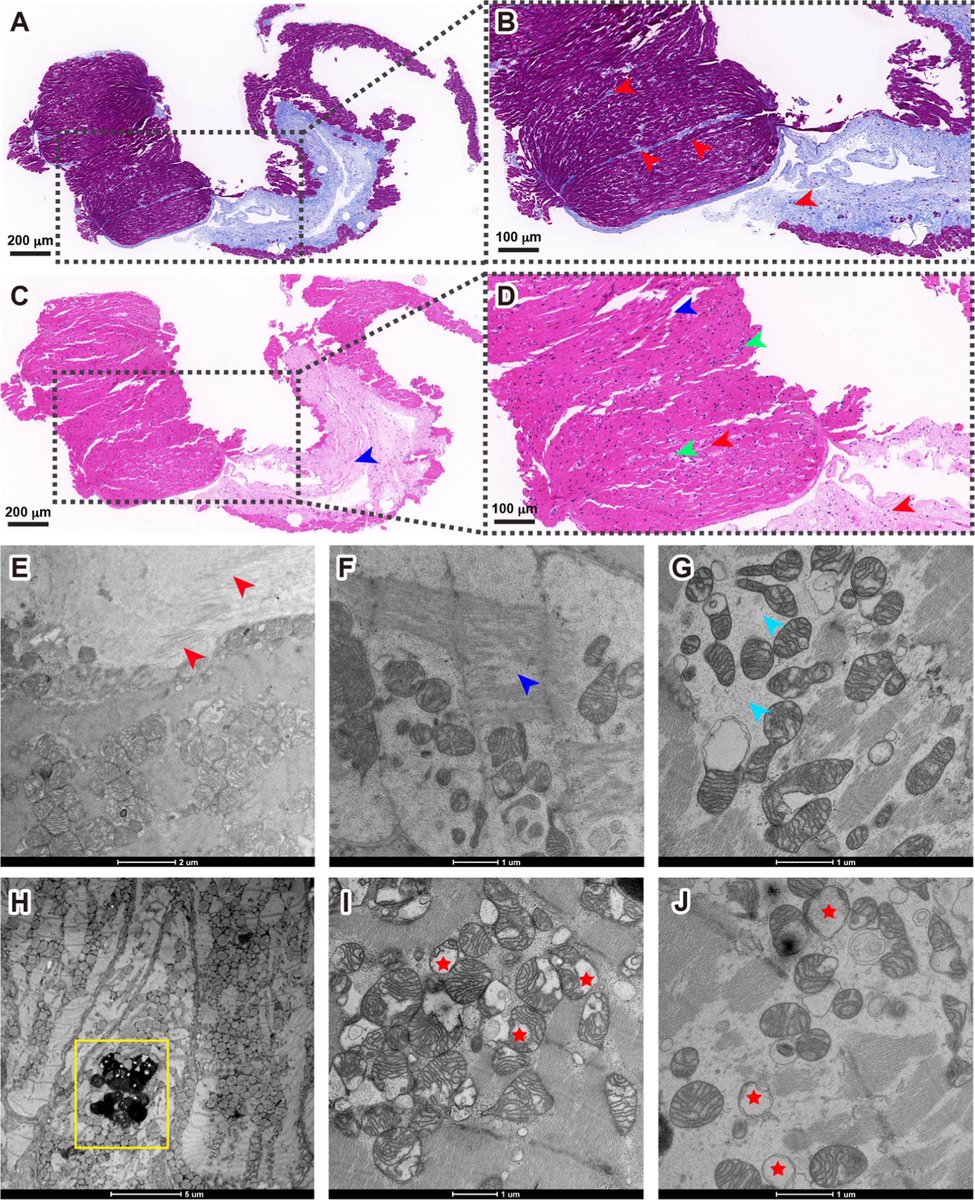
What was so particular about those liver tissues? There was marked hydropic changes of most hepatocytes & ballooning of several, along w/ focal or perivenular necrosis. The diffuse microvesicular fat (seen in Reye’s syn) was absent, not seen in any case. No inflammation 20/


Histological features strongly suggested a dose-related toxic injury. Similarly, on muscle biopsy, degeneration of sarcoplasm w/ loss of striation & hyalinization was seen. Brain biopsies show focal mild giosis, spongiosis & no viral inclusions. 21/




So, the mystery disease got an identity! One disease, multi-system involvement: Pathology in liver, muscle, & brain. Not previously described in humans! Not infectious; not encephalitis nor RS! Then, all 3 of us sat together & coined: #AcuteHeptomyoencephalopathySyndrome 22/

I do not know how many of us get a chance in our lifetime to coin a new disease entity. Probably, we were lucky & the Almighty may have decided to bestow this honor on us! 23/
But the journey was not without hitches. I do not know how the Health administration (& media) got the news of postmortem biopsies. The administration struck back: An FIR was filed ag me; my hospital was sealed & the process to derecognize my degree initiated 24/




That was a very horrid time. I had to face daily harassment from the local administration. There was an intense mental trauma. The administration wanted to push the news related to the outbreak under the carpet & deny existence of any such disease! 25/
I had to shut my hospital & went underground. Luckily, w/ the help of some of my well-wishers, the administration dropped some of the charges. And I could get a sigh of relief. The one lesson that I learned was to keep away from the media..a double-edged sword. 26/
Coming back to the outbreak, which was not over yet. The challenge was to identify the toxin responsible for the disease (Ac HME syndrome). Environmental toxin was strong possibility: affecting only poor kids, narrow age group, peculiar liver histology & no agent identified 27/

At this point, I contacted by childhood buddy, @amodkumartyagi , a community health consultant to carry out epidemiological studies. So, Amod became the fourth member of our team. Meanwhile, we published our major findings in the IJMR in April 2007. 28/
pubmed.ncbi.nlm.nih.gov/17598938/
pubmed.ncbi.nlm.nih.gov/17598938/

With @amodkumartyagi , a case-control study was performed. A very elaborate questionnaire prepared with few pointed Qs on suspected weedy plants. I used to visit affected villages along with my staff on every Sunday. We recorded statements of parents/kids about the incidents. 29/
May have visited at least 100 villages during the ongoing study. We got a hint from a news appeared in DJ paper from the Khekra village where two kids died & several other became sick after consuming a weed. I rushed my lab personnel to visit the village & take samples. 30/

The clinical presentation & lab profile exactly matched the cases we were investigating here. The weed was identified as ‘Pammaad’/‘Kasondi’ (#CassiaOccidentalis). Excitingly, I could not sleep that night. This was the God-sent ‘clue’ 31/

During 2005, 18 cases & 54 controls were included in the study. Positive H/o eating weed was found in 8 cases & in 3 controls. While during 2006 & 07, 57 cases & 169 controls were included, & positive H/o eating Cassia beans was found in 43 cases & amongst only 15 controls. 32/
Parents of 8 (44.4%) cases gave a definite history of their children eating beans of this local, ubiquitous weed #Pamaad (#CassiaOccidentalis) weed before falling ill, compared with 3 (5.6% of 54 controls), the odds ratio being 12.9 (95% CI 2.6-88.8, p<0.001). 33/


The consumption of Cassia beans had a very strong statistical ass w/ onset of #Hepatomyoencephalopathy syndrome (OR 12.89) in 2005; and (OR 31.53) in 2006-07. History of pica was the other associated factor with the disease (OR 5.20) in 2005, and (OR 15.90) in 2006-07. 34/
So, the ‘unknown’ virus of the purported viral encephalitis was unveiled! Cassia occidentalis is a ubiquitous seasonal herb though found in almost every state of the country but grows abundantly, luxuriously in in western UP, UK & neighboring districts of Haryana. 35/

Podding season of #CassiaOccidentalis is from Sept-Nov every year that explains the strong seasonality, recurrences every year, why only rural & peri-urban areas, & why only poor young kids are affected. 36/
Each pod contains around 50-60 beans, juicy during early winter months, tastes like peas. So, the hypothesis of a ‘temperature-labile’ virus by the agencies also got explained by the life cycle of the weed! 37/

Interestingly, not even a single resident of the affected villages was aware of the toxic potential of the weed. In few instances, even grandmother used to feed beans to young kids. 38/
The tender beans were not unpalatable. And this was the reason why young, poor unsupervised kids used to consume a significant quantity of beans while playing. The beans are the most toxic part of the plant and children tend to eat only the beans and no other part. 39/
As with animals, the clinical features depend upon the amount of beans eaten by the children. While consumption of the beans in 2-3 pods by a young child may not have any deleterious impact, a large ‘binge’ can lead to serious disease and death. 40/
As with animals, the clinical features depend upon the amount of beans eaten by the children. While consumption of the beans in 2-3 pods by a young child may not have any deleterious impact, a large ‘binge’ can lead to serious disease and death. 41/
The fatal acute HME syndrome ensues with relatively larger amount of beans - such as what would be equal to a handful in the cupped hand of a child - or a cupful in a toy cup. While most children used to throw them away, some seem to eat the beans. 42/


Lack of parental supervision, children left to themselves, easy access to the plant, plentiful availability, hunger & similarity to other green vegetables seem to be the reasons why children eat the plant.
So, it was a tale of poverty, hunger, ignorance & neglect! 43/
So, it was a tale of poverty, hunger, ignorance & neglect! 43/
There was not a single reference on human toxicity of Cassia occidentalis in literature. In fact, it was labelled as a hepatoprotective in small doses and many Ayurvedic liver tonics like Liv-52, Livomyn, Amlycure, etc contain some amount of this herb. 44/

Extensive literature search was started, and we found many references on animal toxicity. So, animal data showed biological plausibility. 45/

The histopathological & biochemical changes in liver & muscle in animals, died due to Cassia poisoning resemble the features seen in our cases. All the changes occurred in a dose-dependent fashion. We published 2 more papers 46/
pubmed.ncbi.nlm.nih.gov/17684305/
pubmed.ncbi.nlm.nih.gov/17704552/
pubmed.ncbi.nlm.nih.gov/17684305/
pubmed.ncbi.nlm.nih.gov/17704552/


The toxic effects of Cassia beans are dose dependent. According to published reports on animal toxicity, the toxic dose of beans varies from as small as 0.05% to 0.5% of body weight. 47/
A dose as small as 0.05% or 0.5 gm/kg ( 2-3 pods by a 10 kg child) was resp for giving symptoms of cassia poisoning but higher doses 0.2%-0.5% (or 2.0-5.0 gm/kg or 10-25 pods by 10 kg child) would lead to lethal full-blown HME syndrome. 48/
pubmed.ncbi.nlm.nih.gov/19700797/
pubmed.ncbi.nlm.nih.gov/19700797/

Which hepatotoxic toxin was responsible for the massive liver necrosis? The literature hinted toward a group of #Anthraquinons as putative toxin. However, the exact mechanism of action of the toxin was not known. 49/
Earlier it was thought to be through uncoupling of oxidative phosphorylation in mitochondria. However, the most recent theory indicates a high blockade of electron transport (rather than an uncoupling of oxidative phosphorylation) as the chief alteration at cellular level 50/
Coming back to the outbreaks. Following the identification of the weed & its role in the genesis of these recurrent outbreaks, an intense media blitzkrieg was launched. First, we declared our results in a press conference in Saharanpur on July 28, 2007. 51/



Massive educational campaigns were conducted in many districts of western UP & UK with the help of local administration to make people aware of the risk so that future outbreaks may be prevented. 52/




Not only the health dept, but forest dept, PWD, irrigation dept, UNICEF, NPSP & NGOs Rotary, Lions, etc joined hands in educating public about the ill effects of the weed. Even media also helped in creating awareness. 53/




And soon we saw the impact. Within ONE Year of launching educational campaigns all over the affected regions, the cases plummeted significantly 54/


The disappearance of the disease was cited in a paper also! So, we could successfully diagnose & controlled a fatal outbreak that was killing at least 500 kids in many districts of 3 states. And w/out any financial aid from the Govt/agencies 55/
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…

Most of our colleagues, mostly paediatricians working in different districts got convinced with our findings. Few of them could identify the cause-and-effect relationship of Cassia consumption and development of acute HME syndrome. 56/
ijccm.org/doi/IJCCM/pdf/…
ijccm.org/doi/IJCCM/pdf/…




However, the Govt health agencies were still unconvinced of our findings. They were not willing to believe that consumption of a medicinal plant can lead to such a massive & fatal outbreak! 57/
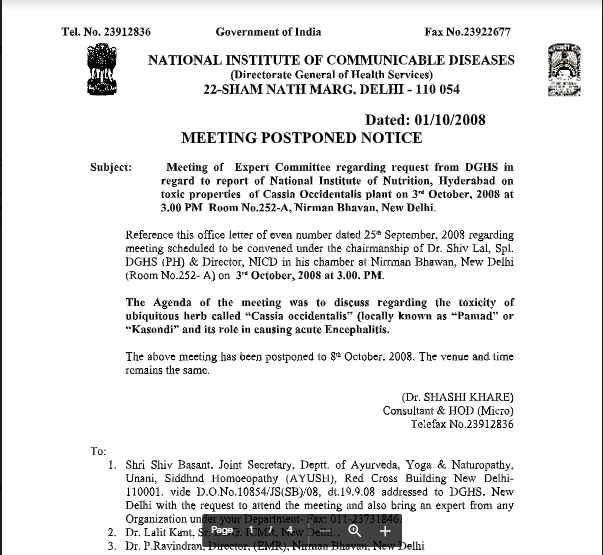
After lot of media pressure, the @MoHFW_INDIA called a meeting on 8th October 2008 at Nirman Bhawan, New Delhi. I along with Dr R K Agarwal (then IAP President) attended this imp meeting & made a presentation on our findings. 58/

As expected, they were quite skeptical of our findings. They kept on finding faults with our hypothesis & the studies. The fellow from NIN, Hyderabad did not present the full study. He simply informed that the bioassay of the weed did not reveal any "neurotoxin". 59/
So, the saga continued….. the onus was on our team to produce an incontrovertible proof of this association & to isolate the exact toxin responsible for the genesis of Ac HME syndrome. Also, to show a cause-and-effect relationship by doing animal and toxicology studies. 60/
I approached many research centres of the country & abroad for toxicology & animal studies: CDRI & ITRC, Lucknow, RRL Jammu, NIN Hyderabad, Urmila Thatte at KEM Mumbai, Sri Ram lab N. Delhi, @CSEINDIA, AIIMS Delhi (Dr Dogra), PGI (Dalbir Singh), CDC Atlanta. 61/
Luckily, Dr Mukul Dass of IITR agreed to collaborate & perform detailed toxicological investigations. The IITR, Lucknow actively associated with us to perform animal & toxicology studies. So, #MukulDass became the fifth member of our team. 62/

Mukul Dass assigned a thesis topic on Cassia-related research to one of his students, G K Panigrahi. They did animal studies (mice). Findings of Cassia consumption showed liver, muscles & brain to be the target organs, which were similar to our clinical data 63/
Overall, their study suggests that Cassia occidentalis (CO) seed consumption is the main etiological factor in children population suffering from Ac HME syndrome in India. 64/
pubmed.ncbi.nlm.nih.gov/24614135/
pubmed.ncbi.nlm.nih.gov/24614135/

Mukul Dass et al also studied the putative mechanism of Cassia induced hepatotoxicity in rats. The results indicated that exposure of CO (0.5%) seeds in diet to rats affected various metabolic pathways. 65/
pubmed.ncbi.nlm.nih.gov/24973489/
pubmed.ncbi.nlm.nih.gov/24973489/

Next was to identify the key toxin/toxic compounds in body fluids of Cassia-exposed patients & experimental rats. The GC-MS analysis of CO seeds revealed the presence of 5 anthraquinones, viz. physcion, emodin, rhein, aloe-emodin, and chrysophanol. 66/
pubmed.ncbi.nlm.nih.gov/25915165/
pubmed.ncbi.nlm.nih.gov/25915165/

Interestingly, these AQs were detected in serum & urine samples from the study cases & CO-exposed rats. Rhein was found the most toxic moiety, followed by emodin, aloe-emodin, physcion, and chrysophanol. 67/
So, in the end, we could identify the KEY TOXIN responsible for the hepatotoxicity and deaths of children—It was #RHEIN ANTHRAQUINONE! 68/
pubmed.ncbi.nlm.nih.gov/25915165/
pubmed.ncbi.nlm.nih.gov/25915165/
Mukul Dass group performed more studies to identify immunomodulatory potential of #Rhein & interaction with DNA & Glutathione. The study concluded that it would be useful in understanding the immune response of CO seeds in human subjects. 69/
pubmed.ncbi.nlm.nih.gov/26784856/
pubmed.ncbi.nlm.nih.gov/26784856/

Taken together, these results suggest that the higher cytotoxicity of Rhein, Emodin and Aloe-emodin may be attributed to their potent DNA and Glutathione (GSH) binding affinity. 70/
pubmed.ncbi.nlm.nih.gov/29326881/
pubmed.ncbi.nlm.nih.gov/29326881/

No, it was not the end of the investigations. Dr Mukul Dass & his team went further to identify a probable antidote to these toxic anthraquinones. It was an immunomodulatory drug known as #CyclosporinA. 71/
It was shown that 100 nM #Cyclosporine A was the most effective among the different protective agents at preventing apoptosis in hepatocytes! Overall, seven toxicology papers were published in peer reviewed journals. 72/
pubmed.ncbi.nlm.nih.gov/25915446/
pubmed.ncbi.nlm.nih.gov/25915446/

Fortunately, or unfortunately, we could not try this compound as an antidote to cassia induced hepatotoxicity owing to almost complete disappearance of these outbreaks by the time this putative antidote was identified! 73/
Fortunately, or unfortunately, we could not try this compound as an antidote to cassia induced hepatotoxicity owing to almost complete disappearance of these outbreaks by the time this putative antidote was identified! 73/
Our team not only did crack the mystery behind these recurring fatal outbreaks and get them controlled with massive educational campaigns, but also provided a probable antidote to treat these almost fatal cases. 75/
en.wikipedia.org/wiki/Acute_HME….
en.wikipedia.org/wiki/Acute_HME….

And we celebrated our ‘victory’ over the dreaded disease in form of a meeting in March 2011 at Saharanpur. This was co-sponsored by the IAP, CHF & ICMR. 76/


This was a landmark study that provided a paradigm shift in the approach of outbreak investigations in India-a fundamental change in approach or underlying assumptions! 77/

Even the @WHO Field Epidemiology Training Programmes (#FETP) of India developed a module based on our approach on how to investigate an outbreak of unknown illness and taught this to young field investigators. 78/

The key findings of our research also solved some of the past ‘puzzles’. I do not know how many of you have heard about ‘Jamshedpur fever’ described by Dr Najeeb Khan in 1954. Or about the Nagpur encephalitis in late 1950s? 79/
Fever w/ altered sensorium in a child is often diagnosed as ‘encephalitis’ by HCW & HCP, without further discrimination. Encephalitis is often attributed to viruses, especially when it occurs in outbreaks. Mind you, the presence of JE in India was discovered in 1955. 80/
Many outbreaks of identical or similar encephalopathy syndrome have occurred in other locations in India, but most of them remained undocumented. Hospital-based studies of outbreaks were reported in several locations in Punjab, Haryana, UP,& Bihar in the mid-&late-1950s. 81/
An outbreak of Reye syndrome in Bangalore during 1983-86. In 1997 there was an outbreak of encephalopathy in children in several districts of Haryana and the adjoining region of Chandigarh. Most of them were classified as Reye-syndrome outbreaks. 82/
pubmed.ncbi.nlm.nih.gov/1818875/
pubmed.ncbi.nlm.nih.gov/1818875/
Can Reye syndrome occur in epidemic form? No, most of these outbreaks were toxin-mediated encephalopathy, & Cassia may be involved in some of them as a toxin. If you are labelling a case as a Reye syndrome, first ascertain that a thorough work-up has been done 83/
An outbreak in 2007 could be identified as toxin mediated in B'desh based on our findings. Some WHO investigators referred our studies to the investigating team in Sylhet. The illness was diagnosed due to consumption of Ghagra shak 84/
pubmed.ncbi.nlm.nih.gov/20305785/
pubmed.ncbi.nlm.nih.gov/20305785/


A large outbreak of similar illness in #Malkangiri town was diagnosed as toxin mediated illness due to consumption of Bada Chakunda, i.e. Cassia in 2014-16. It was acute HME syndrome, and within few hours, Dr TJJ solved this mystery based on our past experience with HME 85/


Then came the recurrent outbreaks of Ac encephalopathy in #Muzaffarpur (2012-19). With the background knowledge gained by working on the Cassia related outbreaks in Saharanpur & other districts, we were sure that this was yet another instance of toxin-mediated outbreak. 86/


In June 2012, we exchanged our thoughts through e-mails, & cracked the mystery behind these outbreaks. On June 24, 2012, I wrote a mail to our group members & IAP colleagues to hint toward role of litchi fruit and the toxin as MCPG responsible for these outbreaks. 87/


Later, Dr TJJ, Mukul Dass and group in 2014-15, published several papers in peer reviewed journals to confirm the role of litchi toxin as a mean reason behind this acute ‘hypoglycaemic encephalopathy’ @PriyankaPulla 88/


I could not be the part of the team because of my preoccupation with some other works & locational disadvantage. Dr TJJ took the charge and along with Dr Arun Shah helped administration to successfully controlled the outbreak there. 89/
These decade long investigations were a great learning exercise. In the process, we learnt several new things. I have just enumerated few here. 90/

Perhaps the greatest lesson was to possess a lateral thinking process-to look at different side! Need to start afresh, w/ open mind w/out any preconceived notion. When the same information is viewed with a diff thought pattern, we get what is known as a paradigm shift 91/
So, have a new look at existing information. Don’t dismiss other point of view recklessly. Before you say, “It cannot be so….”, pause and try to see things from other person’s point of view. Who knows? You may find the rabbit instead of the duck. 92/

Here is the team: Nabeen Nayak, me, TJJ, Amod & Mukul Dass. We didn’t get any official recognition or accolades or award or any felicitation from the state. It was such an enthralling, fulfilling journey that no award can substitute or enhance the value 93/

Whenever, I feel depressed, I go back to the past and try to relive those memories and the time spent together while trying to solve the mystery behind these outbreaks…. And I am not alone. All of us have shared the same thoughts and feelings. 94/
Now, as promised in the beginning of this long thread, the reason why did I choose this time to share this story….has something to do with some recent events…... 95/
During the PEDICON held last month, the organisers, IAP & @BharatBiotech decided to officially felicitate Dr T Jacob John for his lifelong contributions to the science. They also asked me to video record my testimony. 96/
facebook.com/10000165421709…
facebook.com/10000165421709…
facebook.com/10000165421709…
facebook.com/10000165421709…
What can I say about him? TJJ is an institution in himself. Personally, he had a great impact on me. He is the one who introduced me to the world of academics. Whatever little I could achieve, the main credit goes to him. This long tale is indeed my tribute to him... 97/

And this is just one sphere of my association with him. Have worked with him on polio, TB, vaccination, infectious dis etc. But this experience I thought is worth sharing. He asked me several times to start writing a book on this journey. May be, this is just the beginning. 98/
And, yes, I also got an award from my colleagues during the same conference. May be its premature since I do believe, I am not done yet. I still have more to contribute…and may be few more yards (if not miles) to go before I sleep… 99/

In the end, I must acknowledge few of my key associates, colleagues & friends who were the witnesses of this exciting journey: @vibhavarshney , @NiteenWairagkar, @naveenthacker #RSPanwar, Arun Kumar, AjayKalra, @swatibhave , @SunitaNarayana , @shailveesharda, PushpendraSingh 100/
contd @profpiyushgupta @jagchin R K Agarwal, Sudhir Choudhary, Late O P Goel, @BansalCP @iapindia Nita Choudhary, & many more.
And my source of motivation, strength & support my wife @AnjuVashishtha3, my father & kids 101/end
And my source of motivation, strength & support my wife @AnjuVashishtha3, my father & kids 101/end

• • •
Missing some Tweet in this thread? You can try to
force a refresh