
Residents in #Shanghai screaming from high rise apartments after 7 straight days of the city lockdown. The narrator worries that there will be major problems. (in Shanghainese dialect—he predicts people can’t hold out much longer—he implies tragedy).
2) “yao ming le” & “yao si” — both expressions meaning “life and death” but they also more literally means “asking for death”. Narrator eventually implies shit is gonna hit the fan soon if this continues.
3) The video has been verified by @patrickmadrid’s family. It has also been verified by my sources as commonplace. Also, Shanghainese is a local dialect (not really propaganda useful)—only 14 million out of 1.3 billion Chinese even speak. I only speak it because I was born there.
4) China honestly might be hitting a breaking point with #Ba2. Either it keeps going with tragedies growing or it changes direction. See🧵 below. Hunger is growing fast.
https://twitter.com/drericding/status/1512680426015449091
5) The narrator sounds familiar—
Shanghai resident: "I'm breaking through the blockade now—you quickly arrest me, do you have any food to eat in prison?"
Police: "We will arrest you and sent you back. We don't even know where we can buy food outside."
Shanghai resident: "I'm breaking through the blockade now—you quickly arrest me, do you have any food to eat in prison?"
Police: "We will arrest you and sent you back. We don't even know where we can buy food outside."
6) More remarkable in this telephone conversation is how philosophical of a chat the resident and police officer got toward the end. Censors blocked the subtitles—but in Shanghainese the caller gets the cop to think about repercussions for violent rebellion if hunger continues.👇
https://twitter.com/drericding/status/1512691181368619008
7) Of course, Chinese govt doesn’t condone balcony singing or & protesting. And of course, a govt drone appears: “Please comply with COVID rules. **Control your soul’s desire for freedom**. Do not open window to sing.” ➡️yes the drone actually said that.
8) Are people going hungry in Shanghai? Yes. Many people down to one meal a day. You can see here people rationing their vegetables into meal chunks. Dialogue is in Shanghainese, so it’s legit—checks out.
9) There are indeed widespread reports of hunger and food distribution issues. Let’s just suppose it only affects 10% of Shanghai’s 26 million people —that’s still 2.6 million starving. Even if it’s 5% having hunger crisis—that’s still 1.3 million people!
nytimes.com/2022/04/08/wor…
nytimes.com/2022/04/08/wor…
10) Some asked—how can the Chinese government allow millions to go hungry? Well, most Westerners never learned about the horrific **GREAT CHINESE FAMINE** of 1959-1961… in which **up to 55,000,000** (15-55 mil) Chinese starved to death. It’s history.
en.wikipedia.org/wiki/Great_Chi…
en.wikipedia.org/wiki/Great_Chi…
11) The Great Famine “is widely regarded as the deadliest famine & one of the greatest man-made disasters in human history”— death toll of 15-55 million.
📍The % dead in provinces: Anhui (18% dead), Chongqing (15%), Sichuan (13%), Guizhou (11%) and Hunan (8%).
History lessons.
📍The % dead in provinces: Anhui (18% dead), Chongqing (15%), Sichuan (13%), Guizhou (11%) and Hunan (8%).
History lessons.
12) There is a big rich-poor divide in food access. richer neighborhoods have plenty. Food delivery used to cost 30 RMB, but delivery fee now 200-300 RMB! So you can get food—but only you are resourceful enough to find delivery and can afford it even if you do. I’m worried.
13) I think there is definitely a food shortage. Just like we are sure COVID #Ba2 is run amuck in China. The trickier thing is to know how much critical food insecurity / hunger prevalence there is. My family in SH can’t agree—because some life in wealthier parts than others.
14) meanwhile, Police in Shanghai recently started wearing thermal-imaging view screen helmets designed to detect people on the streets with fevers, before lockdown. China is not letting a good crisis goto waste as chance for their surveillance measures.
15) FOOD PRICE GOUGING—in normal times, these veggies would cost 20-30 RMBs. This guy charges 100 RMBs plus 200 RMB delivery fee—300 RMBs—so a ~10x cost increase for food, assuming you can even get delivery. That’s not sustainable for 26 million people.
16) last week, I warned about how Shanghai was at a tipping point. As world financial capital city, Shanghai’s government is desperately trying to stop it before it gets further out of control. But I feared it might be already too late. medriva.com/is-this-shangh…
17) Let this sink in— The U.S. Consulate in Shanghai had to beg for food for US Marines using WeChat. “Marines have depleted their food and can no longer get delivery—if you can spare a meal’s worth or two for 7 extra mouths, they’d be very appreciative” 😳reuters.com/world/china/us…
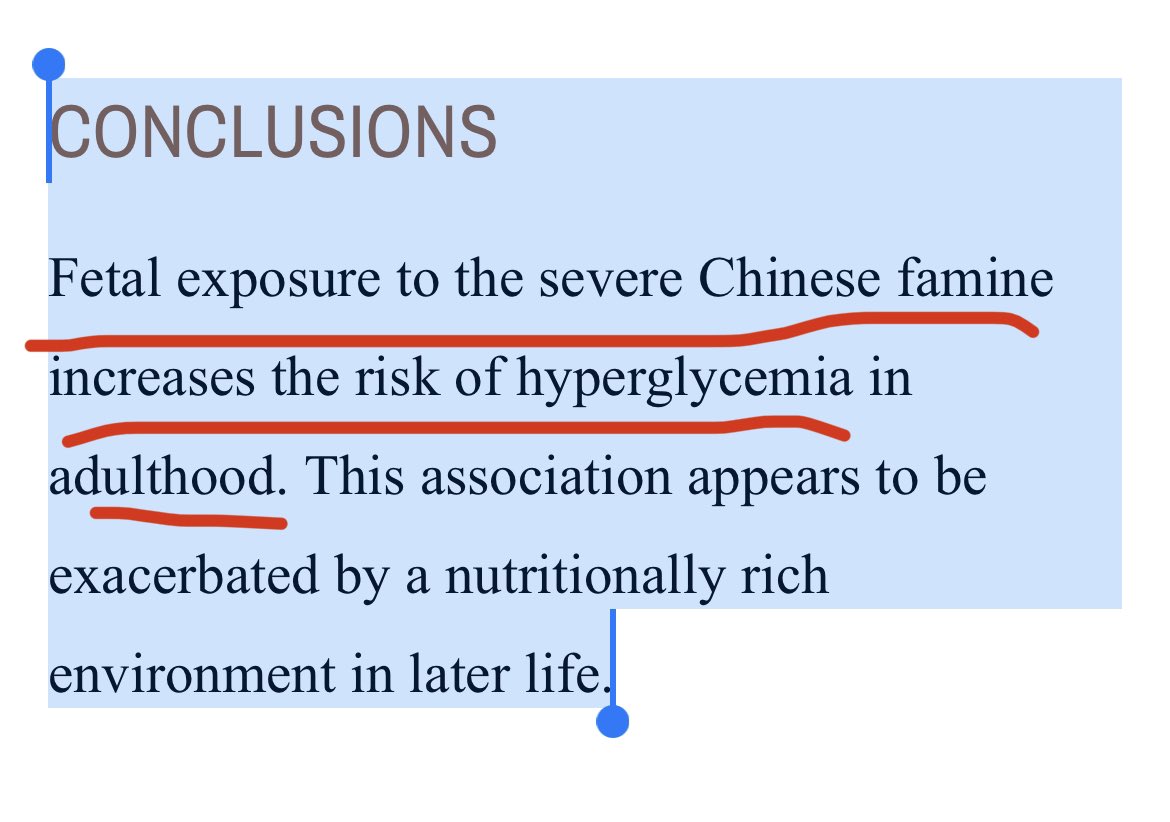
18) What is a long term effect of the Great Chinese Famine—assuming one didn’t die among 15-55 million? Well, my Harvard epidemiology friends did a study—it found fetuses exposed to the famine, later in adulthood, sadly had 4x higher glucose/diabetes risk! ncbi.nlm.nih.gov/pmc/articles/P…
19) Isn’t China good with logistics? Yes, except Chinese daily diet is mostly reliant on unfrozen and unprocessed foods with almost no shelf life. That’s how Chinese diet & food system has been. But that is harder with COVID to deliver than more processed Western diets (ironic?)
https://twitter.com/RealSexyCyborg/status/1512734645384736773
20) Chinese society’s deepest fight is against the humiliation of poverty & hunger. The modern core social contract of CCP is to provide food and prevent mass hunger. If CCP fails to deliver on food to its citizens—that is actually the greatest social failure in Chinese eyes!
https://twitter.com/realsexycyborg/status/1512734612937535491
21) Every Chinese-born person knows this—food is the main way to show both love and hospitality. Even trying to show off there is too much food. Many parents/grandparents who survived the Great Famine (see above) knows that is the hard line that society can never cross again.
22) As @RodZeidan points out in his thread on the food situation in wealthier parts of Pudong, food deliveries are certainly possible — it just take extremely diligent monitoring of food/grocery delivery apps—closing and reopening frequently. Not everyone is that savvy/wealthy.
https://twitter.com/rodzeidan/status/1512782938433556480
23) But elsewhere in the city, there are scenes of looting / mob attacking food shipments too. There are many other small protest videos too— but you get the idea. It’s not everywhere, but it is happening often I’m told.
24) Leaving off with this photoshop of Hunger Games Shanghai. Overall, is the food crisis apocalyptic? No. Are deliveries great? No. Are folks v frustrated? Yes. Even 1-5% of 26 mil is = MANY hungry. But if China loses control—millions may die.
#BA2 is serious & #CovidIsNotOver
#BA2 is serious & #CovidIsNotOver
25) damn, now they are sealing the doors of anyone with a positive case (presumably because the FangCang isolation centers are full).
And this hit home - XuHui District was my grandmother & mom’s childhood home—and one of the key districts of PuXi (west of the river Shanghai).
And this hit home - XuHui District was my grandmother & mom’s childhood home—and one of the key districts of PuXi (west of the river Shanghai).
https://twitter.com/blakestonebanks/status/1513161289719488512
26) But there are reports Shanghai govt is maybe relaxing the “seal you in” approach after pushback. So much is in flux — it’s utter madhouse trying to keep up with the Shanghai govt changes. Follow to keep updated.
https://twitter.com/blakestonebanks/status/1513176231851995138
27) Shanghai seems to have backed off of locking people into their apartment building. But that doesn’t solve the food crisis. Deliveries still sluggish and there’s huge amounts of food waste with produce spoilage outside of Shanghai unable to be delivered into the city.
https://twitter.com/drericding/status/1513510796126523397
28) It looks like Shanghai is solving some of the logistical hurdles for food deliveries. But those without savvy internet skills to order food are at a huge disadvantage and unable to self order food deliveries. And I worry about migrants. @allenwan290
29) I’m seeing comments touting UK 🇬🇧’s mass infection “Let it rip” approach… need I remind you that mass infection will only overwhelm hospitals, which we need for:
Your appendicitis
Your car accident
Your cancer surgery
HCW’s sanity
Or else, you get England 🏴 right now 👇
Your appendicitis
Your car accident
Your cancer surgery
HCW’s sanity
Or else, you get England 🏴 right now 👇
https://twitter.com/drericding/status/1513552049488764929
30) WELP—deniers can no longer deny that the crisis in Shanghai has hit a new level when even the US state department **orders** the evacuation of all Shanghai Consulate non essential employees and family.
Still think it’s just the flu? Still think food crisis not real?
Still think it’s just the flu? Still think food crisis not real?
https://twitter.com/drericding/status/1513685603199631361
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















