Let's talk about Bundled Care of Pediatric Critical Care Patients: Guidelines and Implementation Part 2! We start with Dr. John Berkenbosch talking about choosing the right analgesic/sedation/NMB agent
#SCCM2022 #PedsICU
1/
#SCCM2022 #PedsICU
1/
Underlying disease may cause pain that we cannot well appreciate.
✅Enhancement of sleep should be a goal for its restoration and reduction of delirium.
✅IV opiates strong recommendation to manage moderate to severe pain
❓Need studies comparing opiates
#SCCM2022 #PedsICU
2/
✅Enhancement of sleep should be a goal for its restoration and reduction of delirium.
✅IV opiates strong recommendation to manage moderate to severe pain
❓Need studies comparing opiates
#SCCM2022 #PedsICU
2/

Non-opioid adjunct
Consider use of non opioids both NSAIDS and APAP
Reduced pain scores, and opiate use
#SCCM2022 #PedsICU
3/
Consider use of non opioids both NSAIDS and APAP
Reduced pain scores, and opiate use
#SCCM2022 #PedsICU
3/

But what sedative agents?
✅"Suggest" use alpha2 agonist as primary class of agents
✅alpha agonist used reduced opiate use and reduced incidence of delirium
✅While HR/BP difference, not clinically significant
✅Includes post op cardiac patients
#SCCM2022 #PedsICU
4/
✅"Suggest" use alpha2 agonist as primary class of agents
✅alpha agonist used reduced opiate use and reduced incidence of delirium
✅While HR/BP difference, not clinically significant
✅Includes post op cardiac patients
#SCCM2022 #PedsICU
4/
✅Suggest propofol use limit to less than 48 hours and <4mg/kg/hr
✅More study needed on PRIS
✅NMB-assure use of sedation and analgesia to prevent awareness throughout NMB use
#SCCM2022 #PedsICU
5/
✅More study needed on PRIS
✅NMB-assure use of sedation and analgesia to prevent awareness throughout NMB use
#SCCM2022 #PedsICU
5/
Next Dr. Pete Johnson on right analgesic/sedation agent in the #PedsICU patient
Barriers to optimal selection
🔸drug shortages
🔸patient issues such as renal/hepatic dysfx,
🔸tolerance
🔸obesity dosing adjustments (#whatRDsdo)
#SCCM2022 #PedsICU
6/
Barriers to optimal selection
🔸drug shortages
🔸patient issues such as renal/hepatic dysfx,
🔸tolerance
🔸obesity dosing adjustments (#whatRDsdo)
#SCCM2022 #PedsICU
6/
Given that, ?considerations to build protocols
🔸select pain/sedation scoring tools
🔸select NMB depth/goals
🔸consider unit specific culture in order sets
🔸be aware of JC/CMS med mgmt standards
#SCCM2022 #PedsICU
7/
🔸select pain/sedation scoring tools
🔸select NMB depth/goals
🔸consider unit specific culture in order sets
🔸be aware of JC/CMS med mgmt standards
#SCCM2022 #PedsICU
7/
Barriers and strategies to protocol implementation
🔸changing culture
🔸lack of agreement across providers and disciplines
🔸need multi-pronged education, using champions, online, f2f (ref the SANDWHICH trial)
🔸ongoing vigilance needed for sustainability
#SCCM2022 #PedsICU
8/
🔸changing culture
🔸lack of agreement across providers and disciplines
🔸need multi-pronged education, using champions, online, f2f (ref the SANDWHICH trial)
🔸ongoing vigilance needed for sustainability
#SCCM2022 #PedsICU
8/
Next Dr. Heidi Smith talks about assessment, prevention & mgmt pediatric delirium
🔸prevalence 5-66% in PICU
🔸Hypoactive motor type most common
🔸risk factors incl younger age, neurodev delay, nutrition status, cyanotic CHD
#SCCM2022 #PedsICU #NutritionMatters #PICUNutrition
9/
🔸prevalence 5-66% in PICU
🔸Hypoactive motor type most common
🔸risk factors incl younger age, neurodev delay, nutrition status, cyanotic CHD
#SCCM2022 #PedsICU #NutritionMatters #PICUNutrition
9/
Delirium outcomes include ⬆️LOS, duration MV, ⬆️costs
🔸recommend use of CAPD, pCAM-ICU & psCAM-ICU screening tools
🔸screen routinely throughout PICU stay
🔸
#SCCM2022 #PedsICU
10/
🔸recommend use of CAPD, pCAM-ICU & psCAM-ICU screening tools
🔸screen routinely throughout PICU stay
🔸
#SCCM2022 #PedsICU
10/
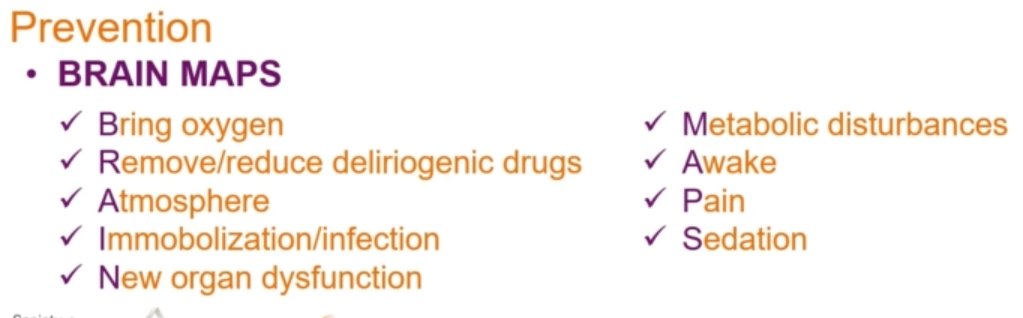
What non-pharm interventions are recommended?
🔸family presence
🔸sleep hygiene
🔸interdisciplinary rounds
🔸early mobility
#SCCM2022 #PedsICU
11/
🔸family presence
🔸sleep hygiene
🔸interdisciplinary rounds
🔸early mobility
#SCCM2022 #PedsICU
11/
Now what pharm interventions are recommended?
🔸what's driving the symptom of agitations?
🔸where is my patient on their illness/recovery trajectory
🔸consider atypical antipsychotics (off label) for agitation, not prevention
🔸minimize use of benzo
#SCCM2022 #PedsICU
12/
🔸what's driving the symptom of agitations?
🔸where is my patient on their illness/recovery trajectory
🔸consider atypical antipsychotics (off label) for agitation, not prevention
🔸minimize use of benzo
#SCCM2022 #PedsICU
12/

Finally, Dr. Shari Simone discusses how to implement delirium screening and what to do with your results!
🔸interdisciplinary task force
🔸measured screening compliance, delirium incidence
🔸#brainrounds monthly conference
#SCCM2022 #PedsICU
13/
🔸interdisciplinary task force
🔸measured screening compliance, delirium incidence
🔸#brainrounds monthly conference
#SCCM2022 #PedsICU
13/
Expect long term work to measure results, institute #QI, and remeasure. Key strategies:
🔸add complexity over time
🔸shared commitment and champions
🔸Buy-in of PICU leadership
🔸Pilot paper screening, then build into EHR
🔸assess knowledge, attitudes
#SCCM2022 #PedsICU
14/14
🔸add complexity over time
🔸shared commitment and champions
🔸Buy-in of PICU leadership
🔸Pilot paper screening, then build into EHR
🔸assess knowledge, attitudes
#SCCM2022 #PedsICU
14/14

• • •
Missing some Tweet in this thread? You can try to
force a refresh