1/
Awhile ago, on a triage call: “I’ve got a guy here, pretty young, came in looking terrible. GCS 4, we intubated him. Scan shows a big bleed. ICH score 4. Not sure much you’ll be able to do, but need to transfer him.”
A #tweetorial about the ICH score. @medtweetorials
Awhile ago, on a triage call: “I’ve got a guy here, pretty young, came in looking terrible. GCS 4, we intubated him. Scan shows a big bleed. ICH score 4. Not sure much you’ll be able to do, but need to transfer him.”
A #tweetorial about the ICH score. @medtweetorials


2/
When you hear ICH score 4 you think...
When you hear ICH score 4 you think...
3/
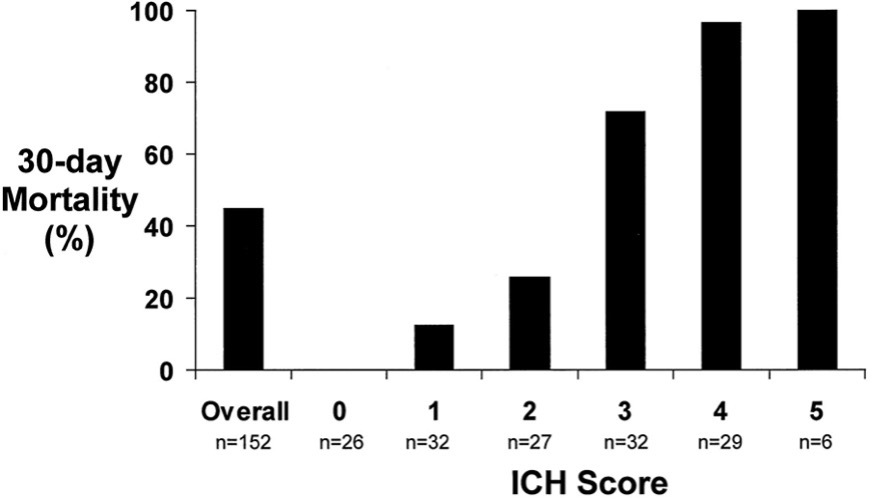
97% morality was associated with Score 4 in the original paper (pubmed.ncbi.nlm.nih.gov/11283388/)
The score, developed to be a reliable/easy to calc severity index, was determined from a
👉 Retrospective cohort
👉 By logistic regression analysis of independent predictors of mortality
97% morality was associated with Score 4 in the original paper (pubmed.ncbi.nlm.nih.gov/11283388/)
The score, developed to be a reliable/easy to calc severity index, was determined from a
👉 Retrospective cohort
👉 By logistic regression analysis of independent predictors of mortality
4/
I hear you thinking… that scan isn’t THAT bad.
ICH 4? ... Really?
➡️Reported GCS 4 (M2E1V1): extensor posturing, not opening eyes or verbalizing. (+2 pt)
➡️Bleed ~40cc (+1)
➡️IVH (+1)
Check for yourself: mdcalc.com/intracerebral-…
I hear you thinking… that scan isn’t THAT bad.
ICH 4? ... Really?
➡️Reported GCS 4 (M2E1V1): extensor posturing, not opening eyes or verbalizing. (+2 pt)
➡️Bleed ~40cc (+1)
➡️IVH (+1)
Check for yourself: mdcalc.com/intracerebral-…
5/
At the time of arrival to our ICU, however, the patient could open eyes to noxious stim and was withdrawing on the left (6T).
Sometimes we get things that are way worse than billed, but this is clearly better.
Was the first exam just wrong??
At the time of arrival to our ICU, however, the patient could open eyes to noxious stim and was withdrawing on the left (6T).
Sometimes we get things that are way worse than billed, but this is clearly better.
Was the first exam just wrong??
6/
I doubt it. (I wasn’t there, but I do trust this was the exam).
A reminder that everyone looks terrible when:
🚫Airway protection
✅Aspirating
+/- hypercarbia
Reminder: pH ⬇️ ▶️ vasodilation ▶️ more CBF ▶️
⬆️ ICP =
I doubt it. (I wasn’t there, but I do trust this was the exam).
A reminder that everyone looks terrible when:
🚫Airway protection
✅Aspirating
+/- hypercarbia
Reminder: pH ⬇️ ▶️ vasodilation ▶️ more CBF ▶️
⬆️ ICP =
7/
Just with intubation, things are better.
After an EVD was placed:
👁️ Eyes opening to voice
👍 Mimicking commands on the left (9T)
Simple interventions. Basic resuscitation. And the patient more doubled their GCS and downshifted their ICH Score by 1 pt.
Just with intubation, things are better.
After an EVD was placed:
👁️ Eyes opening to voice
👍 Mimicking commands on the left (9T)
Simple interventions. Basic resuscitation. And the patient more doubled their GCS and downshifted their ICH Score by 1 pt.
8/
But since the ICH Score is the most commonly used score and required documentation by #TheJointCommission, there are some rules. The earliest score counts.
The manual states the score should be calc BEFORE surgical intervention.
tinyurl.com/y8uf624r
But since the ICH Score is the most commonly used score and required documentation by #TheJointCommission, there are some rules. The earliest score counts.
The manual states the score should be calc BEFORE surgical intervention.
tinyurl.com/y8uf624r

9/
Ok. Maybe we all agree that an ICH score 3 sounds a bit more like it fits here, but the associated mortality is still:
Ok. Maybe we all agree that an ICH score 3 sounds a bit more like it fits here, but the associated mortality is still:
10/
ICH score 3, from the original paper, had an associated 72% 30-day mortality.
So...tell the family “Your loved one has a 72% chance of being dead in 30 days”?
Tell them even more dismal data associated with the initial score of 4 since that's what's in the chart?
ICH score 3, from the original paper, had an associated 72% 30-day mortality.
So...tell the family “Your loved one has a 72% chance of being dead in 30 days”?
Tell them even more dismal data associated with the initial score of 4 since that's what's in the chart?
11/
Please do neither!!
(and not just because that would be a terribly insensitive way to say things...)
‼️‼️The ICH score what NEVER meant to be an acute prognosis tool‼️‼️
‼️‼️The ICH score what NEVER meant to be an acute prognosis tool‼️‼️
Please do neither!!
(and not just because that would be a terribly insensitive way to say things...)
‼️‼️The ICH score what NEVER meant to be an acute prognosis tool‼️‼️
‼️‼️The ICH score what NEVER meant to be an acute prognosis tool‼️‼️
12/
The ICH scale was developed as a framework for clinical decision making and to stratify/ standardized communication.
An ICH score of 4 is a more severe injury than an ICH score of 3; that’s been validated in global cohorts and that’s useful knowledge in planning treatment.
The ICH scale was developed as a framework for clinical decision making and to stratify/ standardized communication.
An ICH score of 4 is a more severe injury than an ICH score of 3; that’s been validated in global cohorts and that’s useful knowledge in planning treatment.
13/
So, why not use it for prognostication about death?
To answer that… another question:
“why do patients with ICH die?”
So, why not use it for prognostication about death?
To answer that… another question:
“why do patients with ICH die?”
14/
I can think of some ways:
👉Progression to brain death
👉Mucus plugging
👉Sepsis
👉PE
But *by far*, the most common cause of death is withdrawal of life support.
In later studies ~80% of pt who died in the hospital, died of WLST. pubmed.ncbi.nlm.nih.gov/19726752/
I can think of some ways:
👉Progression to brain death
👉Mucus plugging
👉Sepsis
👉PE
But *by far*, the most common cause of death is withdrawal of life support.
In later studies ~80% of pt who died in the hospital, died of WLST. pubmed.ncbi.nlm.nih.gov/19726752/
15/
As clinicians caring for ICH pts, the prognosis we give to the family has the most significant impact on the decision of whether to continue aggressive care.
This “self-fulfilling prophecy” is inherent to the score (WLST was allowed in the cohort) and reinforced by it.
As clinicians caring for ICH pts, the prognosis we give to the family has the most significant impact on the decision of whether to continue aggressive care.
This “self-fulfilling prophecy” is inherent to the score (WLST was allowed in the cohort) and reinforced by it.
16/
Take this case.
If we told the family "nearly all patients with this initial severity of injury do not survive the first month", most families hear, "Nothing can be done. This is not survivable." And withdraw care.
But with maximal care, there's a different outcome.
Take this case.
If we told the family "nearly all patients with this initial severity of injury do not survive the first month", most families hear, "Nothing can be done. This is not survivable." And withdraw care.
But with maximal care, there's a different outcome.
17/
Anecdotes are great; data is better.
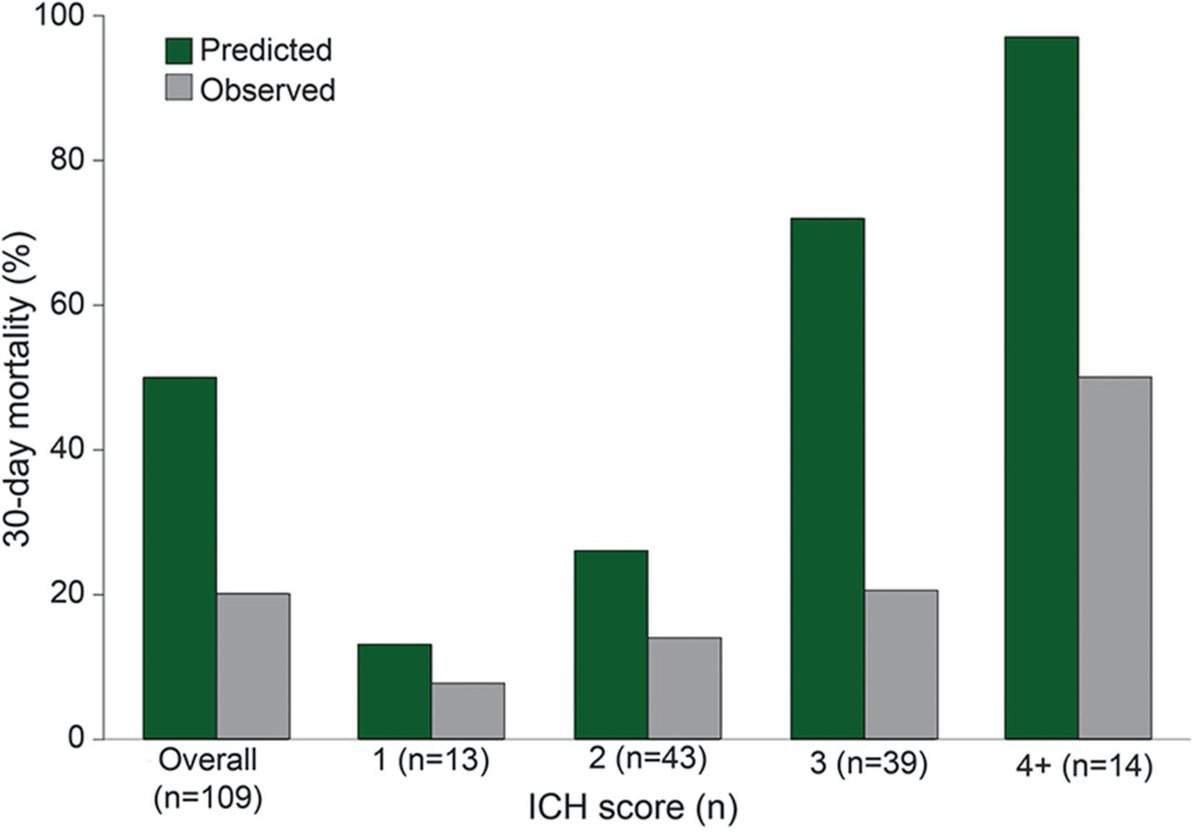
Led by the ICH Score authors: In a study of pts in who agreed to withhold a DNR / withdrawal of life support within the first 5 days, the same thing is seen:
30 day outcome is much better than predicted.
pubmed.ncbi.nlm.nih.gov/25817842/
Anecdotes are great; data is better.
Led by the ICH Score authors: In a study of pts in who agreed to withhold a DNR / withdrawal of life support within the first 5 days, the same thing is seen:
30 day outcome is much better than predicted.
pubmed.ncbi.nlm.nih.gov/25817842/
18/
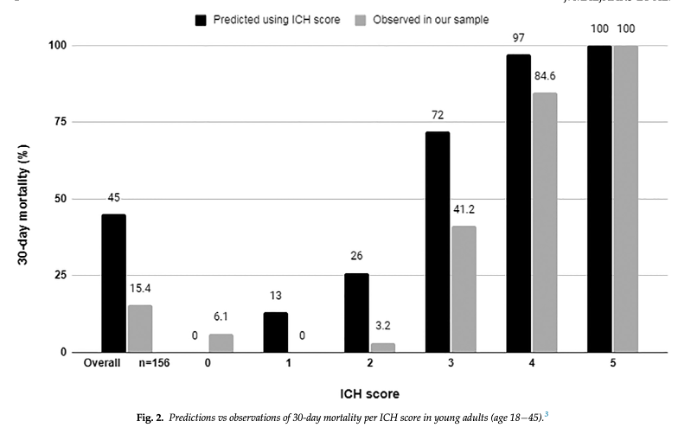
Retrospective data has also suggested the ICH score may overpredict mortality in young patients (<45 year old).
pubmed.ncbi.nlm.nih.gov/34247055/
Retrospective data has also suggested the ICH score may overpredict mortality in young patients (<45 year old).
pubmed.ncbi.nlm.nih.gov/34247055/
19/
I would love to tell you: “this patient is doing great!” but, an honest assessment would be that they have achieved what the family feels is reasonable quality of life. There is significant disability. It has been a really long road.
We continue to need better tx for ICH.
I would love to tell you: “this patient is doing great!” but, an honest assessment would be that they have achieved what the family feels is reasonable quality of life. There is significant disability. It has been a really long road.
We continue to need better tx for ICH.
20/
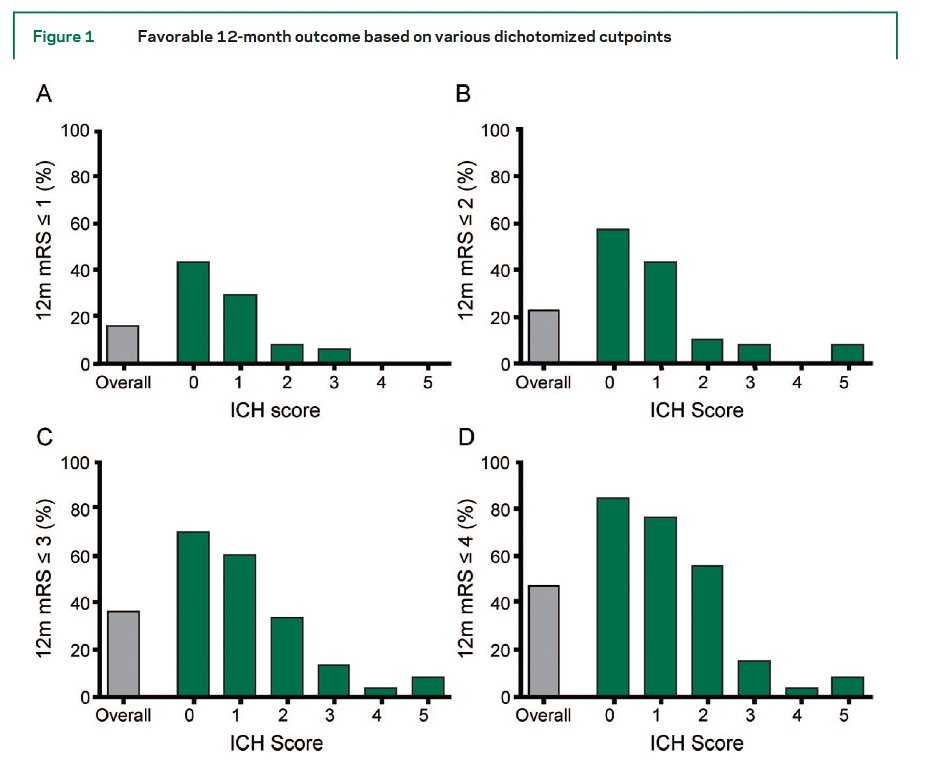
But this case's outcome does mirror later studies of the ICH score, which have demonstrated that higher ICH scores are:
👉Associated w/ higher rates of disability at 12m;
but, also:
👉That improvement is possible even months after discharge
But this case's outcome does mirror later studies of the ICH score, which have demonstrated that higher ICH scores are:
👉Associated w/ higher rates of disability at 12m;
but, also:
👉That improvement is possible even months after discharge
21/
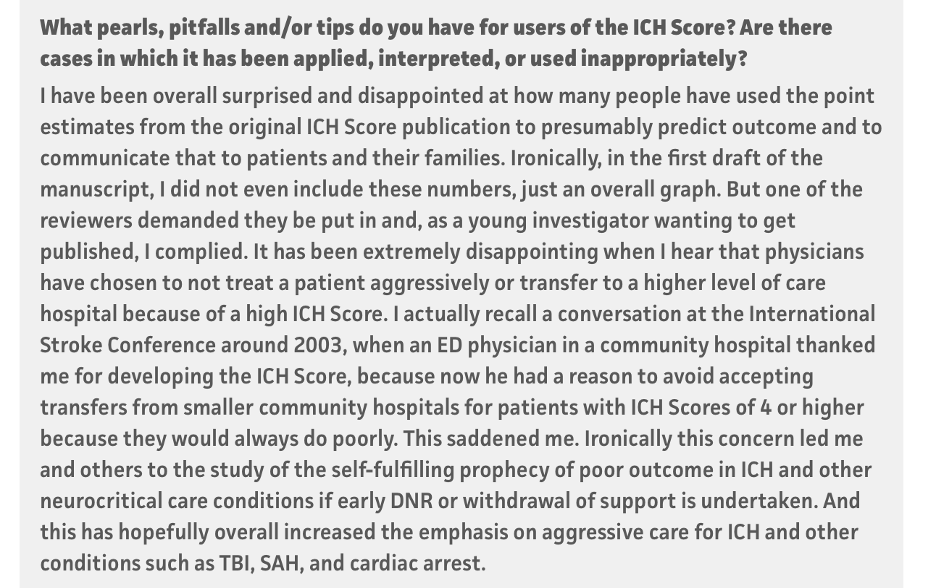
So it isn’t that the ICH score is meaningless.
It’s just that it was never meant to be the determination of who gets aggressive care and who gets withdrawal of life support.
This is not a secret!
It's beautifully written out by @ClaudeHemphill right on MDcalc:
So it isn’t that the ICH score is meaningless.
It’s just that it was never meant to be the determination of who gets aggressive care and who gets withdrawal of life support.
This is not a secret!
It's beautifully written out by @ClaudeHemphill right on MDcalc:
22/
But, I think unfortunately, this may get overlooked because it’s just so easy to triage based on a number.
At the end of the day, prognostication is HARD. But, even so, work by @davidyhwang shows clinicians are still better than algorithms
ncbi.nlm.nih.gov/pmc/articles/P…
But, I think unfortunately, this may get overlooked because it’s just so easy to triage based on a number.
At the end of the day, prognostication is HARD. But, even so, work by @davidyhwang shows clinicians are still better than algorithms
ncbi.nlm.nih.gov/pmc/articles/P…
23/
And, finally, this is not to argue that every patient with an ICH score of 4 should have everything done.
Similar to the post about large strokes & DHC-- context, patient values, and the resources available matter.
But, that decision should be based on more than a number
And, finally, this is not to argue that every patient with an ICH score of 4 should have everything done.
Similar to the post about large strokes & DHC-- context, patient values, and the resources available matter.
But, that decision should be based on more than a number
24/
Take-aways:
✨Intubation and EVDs can do wonders for a GCS (resuscitate first, prognosticate later unless GOC don't support that)
✨The ICH score is a great tool for conveying the initial severity of bleed to other clinicians, not for "treat vs NTD"
Take-aways:
✨Intubation and EVDs can do wonders for a GCS (resuscitate first, prognosticate later unless GOC don't support that)
✨The ICH score is a great tool for conveying the initial severity of bleed to other clinicians, not for "treat vs NTD"
25/
✨Context matters (@drdangayach & I talked a lot about this in #HR22) but ICH Score 4 means a LOT to do!! Both in terms of understanding wishes and potentially in interventions.
🙏@sigman_md for peer-reviewing
@CuringComa @emcrit @CajalButterfly @aartisarwal @SWahlster
✨Context matters (@drdangayach & I talked a lot about this in #HR22) but ICH Score 4 means a LOT to do!! Both in terms of understanding wishes and potentially in interventions.
🙏@sigman_md for peer-reviewing
@CuringComa @emcrit @CajalButterfly @aartisarwal @SWahlster
@namorrismd @nsanar @PulmCrit @rkchoi @a_charidimou @AvrahamCooperMD @pouyeah @neurocritical @neurologyrules @JayKinariwala @theABofPharmaC @ghoshal_shivani @AaronLBerkowitz @aszelikovich @Tracey1milligan @JimmySuhMD @CaseyMayPharmD @EmoryNeuroCrit
• • •
Missing some Tweet in this thread? You can try to
force a refresh