Why are medical podcasts like @thecurbsiders, @BehindTheKnife, @emcrit, and @AFPpodcast so popular for learning? And who is making them? And can they be trusted?
We listened to (and coded) the top 100 podcasts on the Apple podcasts US medicine chart to find out!
A 🧵⬇️
We listened to (and coded) the top 100 podcasts on the Apple podcasts US medicine chart to find out!
A 🧵⬇️

There were 2⃣ inspirations for this study.
@ShreyaTrivediMD and I at @iMedEducation think that what makes digital education unique from eg an uploaded lecture on YouTube is that that it is produced as part of a virtual community of practice and not traditional institutions.
@ShreyaTrivediMD and I at @iMedEducation think that what makes digital education unique from eg an uploaded lecture on YouTube is that that it is produced as part of a virtual community of practice and not traditional institutions.

So we had a hypothesis: the most popular medical podcasts would *not* be produced by medical schools, residency programs, or other large institutions, but rather by individuals (or separate companies/nonprofits).
The second question was inspired by @sargsyanz and @HollandKaplan in this great article in @JournalofGME: ncbi.nlm.nih.gov/pmc/articles/P….
Medical podcasts are basically like lectures WITHOUT the visuals, yet people listen to HOURS of them a week. What possibly makes people do that??
Medical podcasts are basically like lectures WITHOUT the visuals, yet people listen to HOURS of them a week. What possibly makes people do that??
How do we even identify the top podcasts?? (it's a real methodological problem since podcasts are pre-Web2.0 and don't share download data). In order to do this we partnered with @ChartableDotCom and @dzohrob to calculate the top 100 podcasts in medicine in the US over 28 months.
After that, @nicolastrad, Ellen Zhang, and I painstakingly validated a code book looking at didactic method, creators, audience, advertisers, citations/references and more! Then we sat down and listened to, and coded *500* podcast eps!
It took a long time (don't worry, we didn't listen to ENTIRE episodes -- but we each listened to ~14 hours of audio each). @rwcorty is the type of person who unwinds with some large data sets and R, and he set about analyzing the data.
The TL;DR -- our hypotheses were right.
2/3 of podcasts are created by individuals or companies. Less than 10% are created by traditional institutions.
@sargsyanz et al were right too -- popular podcasts DO actually use more active learning/adult learning theory.
2/3 of podcasts are created by individuals or companies. Less than 10% are created by traditional institutions.
@sargsyanz et al were right too -- popular podcasts DO actually use more active learning/adult learning theory.
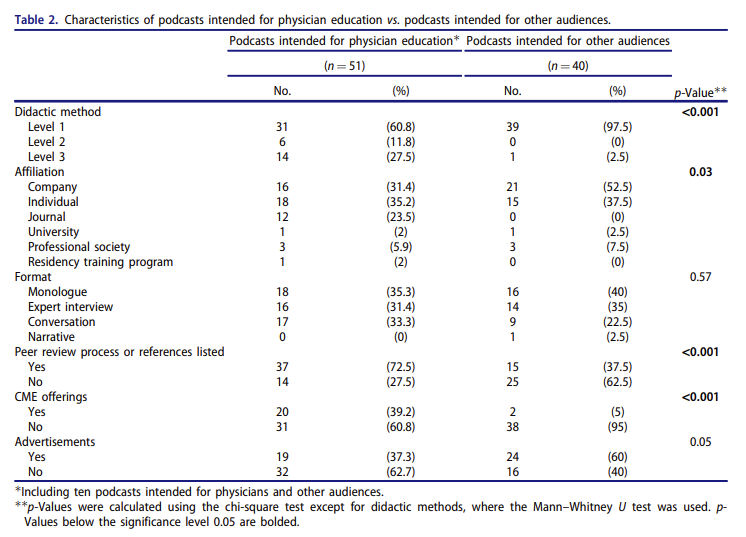
Other interesting findings: inclusion of references is common (73%); 37% of medical podcasts for physicians have advertising; most podcasts target a broad audience of learners from students to attendings.
There were also significant differences in how podcasts intended for physicians taught from those intended for other health professions (or the general public).
If you want to dig through the data yourself, you can access our study at @MedTeachJournal: pubmed.ncbi.nlm.nih.gov/35531609/
There are *lots* of limitations to our study (I won't belabor them in a Twitter thread). But I think it's an important contribution to digital education literature because:
1⃣ It seeks to COMPREHENSIVELY look at the top podcasts using a data-driven approach
1⃣ It seeks to COMPREHENSIVELY look at the top podcasts using a data-driven approach
2⃣ It lends credence towards many of the theoretical arguments that @ShreyaTrivediMD and I make about what makes digital education different and special
3⃣ It gives signals about future directions of this sort of research -- especially investigating review processes and ads
3⃣ It gives signals about future directions of this sort of research -- especially investigating review processes and ads
That's it for the thread! I genuinely enjoyed working on this study, and couldn't have done with without a great team, especially students/co-first authors/podcast-listener-coders Ellen Zhang and @nicolastrad.
And if this gets you excited about digital education, then get even more excited -- because the annual @iMedEducation national meeting will be back on October 7-8. Details will be coming soon!
• • •
Missing some Tweet in this thread? You can try to
force a refresh