Paediatric hepatitis twitter is a little wild at the moment
As a result, there is a lot of stuff circulating which is totally incorrect
Whilst there's much we don't know, there is some stuff we KNOW is not true
A short thread to bust some myths 💥
1/ 🧵
As a result, there is a lot of stuff circulating which is totally incorrect
Whilst there's much we don't know, there is some stuff we KNOW is not true
A short thread to bust some myths 💥
1/ 🧵
The important take-away is that these cases COULD be linked to #COVID19 and this must be investigated, but there is little certainty over *any* of the current hypotheses
Lots of people however seem certain it is related to covid, and therefore false links have been made
2/
Lots of people however seem certain it is related to covid, and therefore false links have been made
2/
First, a recent paper from Japan purports to show an epidemiological link between Omicron and cases of paediatric hepatitis
It actually just shows big countries have more people, and more people means more cases of #COVID19 and hepatitis
See thread
3/
It actually just shows big countries have more people, and more people means more cases of #COVID19 and hepatitis
See thread
3/
https://twitter.com/apsmunro/status/1525164612735344640?s=20&t=wr6WS5sgKbv3Lxy_S6PGJw
People are also sharing cases of #COVID19 causing hepatitis in other children as if this is proof
These are categorically NOT what is happening in the current outbreak, as acute covid hepatitis is easy to diagnose, and most cases are not covid +ve
4/
journals.lww.com/jpgn/Abstract/…
These are categorically NOT what is happening in the current outbreak, as acute covid hepatitis is easy to diagnose, and most cases are not covid +ve
4/
journals.lww.com/jpgn/Abstract/…
A case of post-covid autoimmune hepatitis is being shared as if this is an explanation
This case was diagnosed by anti-lkm antibodies, a test for autoimmune hepatitis which should be done on all cases, and if +ve would EXCLUDE them from the outbreak
5/
ncbi.nlm.nih.gov/pmc/articles/P…
This case was diagnosed by anti-lkm antibodies, a test for autoimmune hepatitis which should be done on all cases, and if +ve would EXCLUDE them from the outbreak
5/
ncbi.nlm.nih.gov/pmc/articles/P…
This is VERY important - the case definition means that causes such as autoimmune hepatitis and acute covid hepatitis would explicitly be excluded from this outbreak analysis
It is puzzling precisely because these causes are being investigated and have not been found
6/
It is puzzling precisely because these causes are being investigated and have not been found
6/
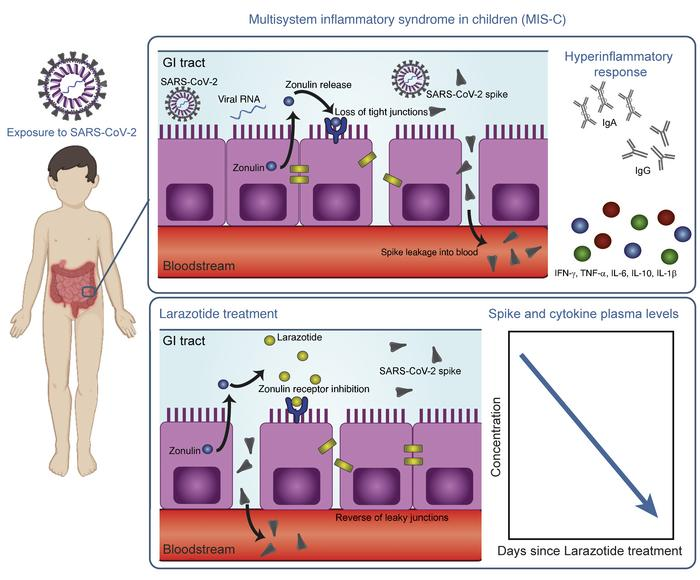
Now @BrodinPetter has proposed a very elegant hypothesis in Adenovirus triggering activation of intestinal reservoir of #SARSCoV2 and subsequent superantigen stimulated liver disease
This has no supporting evidence *yet*, but needs investigating
7/
This has no supporting evidence *yet*, but needs investigating
7/
https://twitter.com/BrodinPetter/status/1525246188404060161?s=20&t=wr6WS5sgKbv3Lxy_S6PGJw
It's worth noting the hypothesis leans on the hypothesis of a similar mechanism behind MIS-C
This is based on work showing S antigen in blood of MIS-C patients in a study from Massachusetts
However...
8/
jci.org/articles/view/…
This is based on work showing S antigen in blood of MIS-C patients in a study from Massachusetts
However...
8/
jci.org/articles/view/…
A separate study from Boston children's hospital with a larger sample size did not replicate this finding, despite antigen being present in blood of children with acute #COVID19
This doesn't rule it out, but shows the case is far from cut and dry
9/
pubmed.ncbi.nlm.nih.gov/35213684/
This doesn't rule it out, but shows the case is far from cut and dry
9/
pubmed.ncbi.nlm.nih.gov/35213684/
The reason these cases are noteworthy is there is *no obvious cause*
As described elsewhere, Adenovirus 41 appears so frequently to raise suspicion, but wouldn't normally cause this kind of disease
Everything is on the table, but needs investigating carefully, without bias
10/
As described elsewhere, Adenovirus 41 appears so frequently to raise suspicion, but wouldn't normally cause this kind of disease
Everything is on the table, but needs investigating carefully, without bias
10/
I won't go into all the potential hypotheses here as it's not the point, and there are plenty of good documents from @UKHSA, @ECDC_EU and @CDCgov
My advice would be: anyone who suggests the cause is obvious is not a trustworthy source of information on this topic
11/end
My advice would be: anyone who suggests the cause is obvious is not a trustworthy source of information on this topic
11/end
• • •
Missing some Tweet in this thread? You can try to
force a refresh