#POCUS #VExUS consult for #hyponatremia. Elderly pt with h/o mitral valve replacement. On Bumetanide, UNa ~70 mmol/L, Uosm ~250🧵
Trace edema, JVD +, feels OK
Calling hemodynamic friends @khaycock2 @ThinkingCC @ArgaizR @msiuba @IM_Crit_ @MDBeni @siddharth_dugar Educate us!
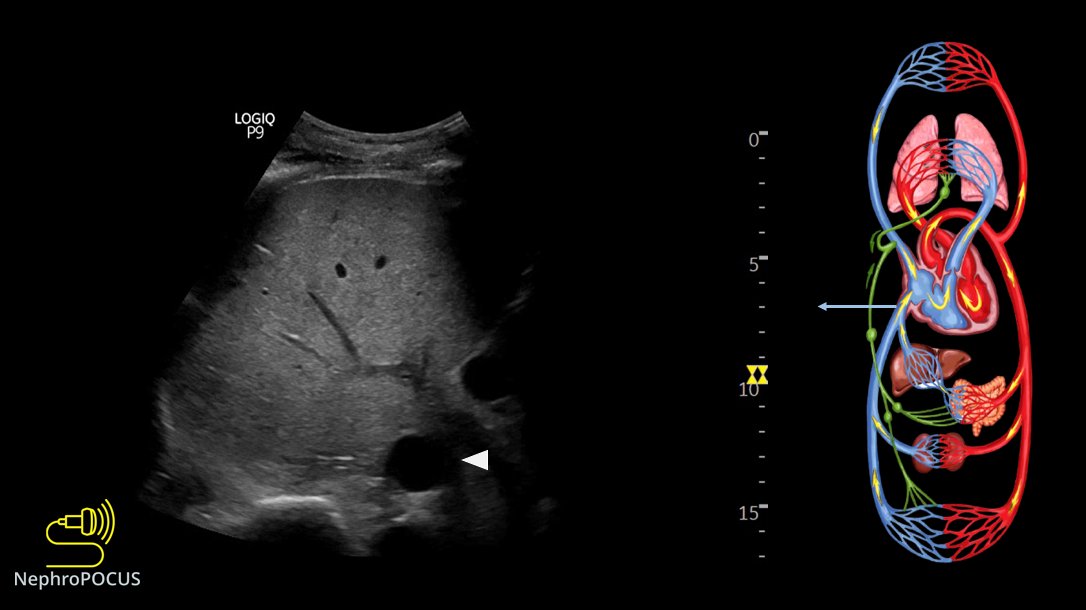
1/ IVC
Trace edema, JVD +, feels OK
Calling hemodynamic friends @khaycock2 @ThinkingCC @ArgaizR @msiuba @IM_Crit_ @MDBeni @siddharth_dugar Educate us!
1/ IVC
2/ 👆Consistent with elevated right atrial pressure.
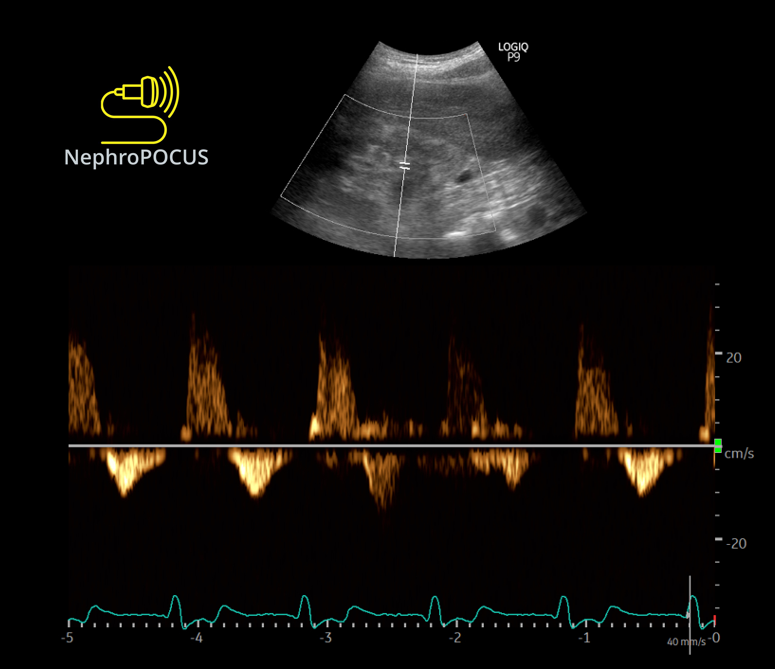
👇Hepatic vein #VExUS
D-only pattern (rhythm: ventricular paced)
👇Hepatic vein #VExUS
D-only pattern (rhythm: ventricular paced)


4/ Intra-renal
D-only as expected (underlying CKD stage IIIb - IV)
D-only as expected (underlying CKD stage IIIb - IV)
5/ Lungs
Predominantly A-lines, occasional B-lines, but no more than 2 per rib interspace
Representative image👇
Predominantly A-lines, occasional B-lines, but no more than 2 per rib interspace
Representative image👇
6/ So far, venous limb is consistent with congestion/elevated RAP.
Minimally elevated extravascular lung water.
Going to the 🫀
@MDBeni can you please share some pearls for #POCUS users when evaluating prosthetic MV🙏
What you think of this?
Minimally elevated extravascular lung water.
Going to the 🫀
@MDBeni can you please share some pearls for #POCUS users when evaluating prosthetic MV🙏
What you think of this?
7/ 👆Both atria are big; particularly LA with bowing of IAS to the right.
Qualitatively, would you 'suspect' MV stenosis?
👇Gradient across MV. What does this tell?
Qualitatively, would you 'suspect' MV stenosis?
👇Gradient across MV. What does this tell?

8/ LV EF looks OK qualitatively.
Let's get LVOT VTI
Looks very high👇
(as you may have noted, there are multiple sample gates; they are automatically appearing when I increase the scale🤦♂️)
Let's get LVOT VTI
Looks very high👇
(as you may have noted, there are multiple sample gates; they are automatically appearing when I increase the scale🤦♂️)

9/ As we must take avg. of 3-4 readings, lets see one more. All 4 were similar.

10/ Why VTI is high?🤔
Maybe I should get CWD of LVOT. AS?
👇What does this tell?
Maybe I should get CWD of LVOT. AS?
👇What does this tell?

11/ Forgot to mention about TR.
Its trace-mild. Couldn't get a good envelope.
Its trace-mild. Couldn't get a good envelope.
12/
OK, what can this nephrologist with limited #POCUS skills infer from the above?🤔
Cc @katiewiskar @ria_dancel @Rajiv_Sinanan @Tubulocentric
OK, what can this nephrologist with limited #POCUS skills infer from the above?🤔
Cc @katiewiskar @ria_dancel @Rajiv_Sinanan @Tubulocentric
• • •
Missing some Tweet in this thread? You can try to
force a refresh