1/ Is the voice box a black box for you?! Let's open the pandora's box of the anatomy of the #larynx together
An introductory #tweetorial on laryngeal #anatomy and the supporting structures. #FOAMed #medtwitter #meded #neurorad #HNrad #FOAMrad #medstudenttwitter @MedTweetorials
An introductory #tweetorial on laryngeal #anatomy and the supporting structures. #FOAMed #medtwitter #meded #neurorad #HNrad #FOAMrad #medstudenttwitter @MedTweetorials

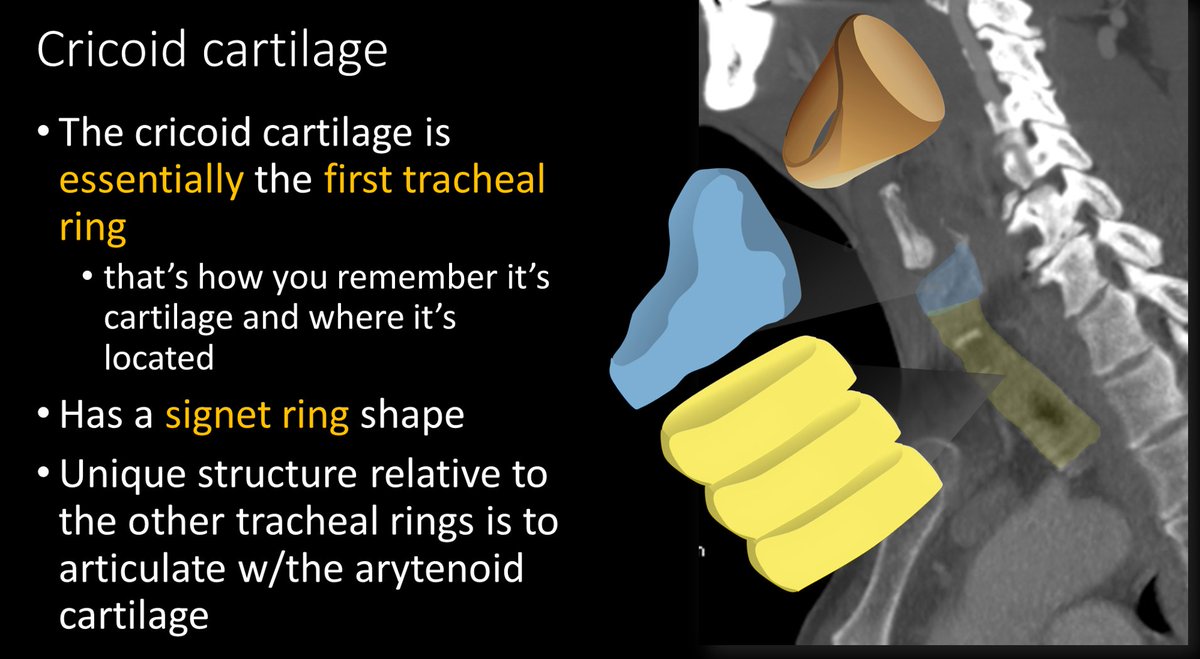
2/Everyone needs some support. Just like the tongue is supported by the hyoid, the main laryngeal support is the cricoid cartilage. It's like your favorite chair, with all the remotes next to it--not only does the cricoid provide support, it also connects structures in the larynx

3/ Although not official, the cricoid is like the real first ring of the trachea. Except it has an odd signet ring shape. The bulbous back part that makes it look like a signet ring provides the important articulation with the arytenoids
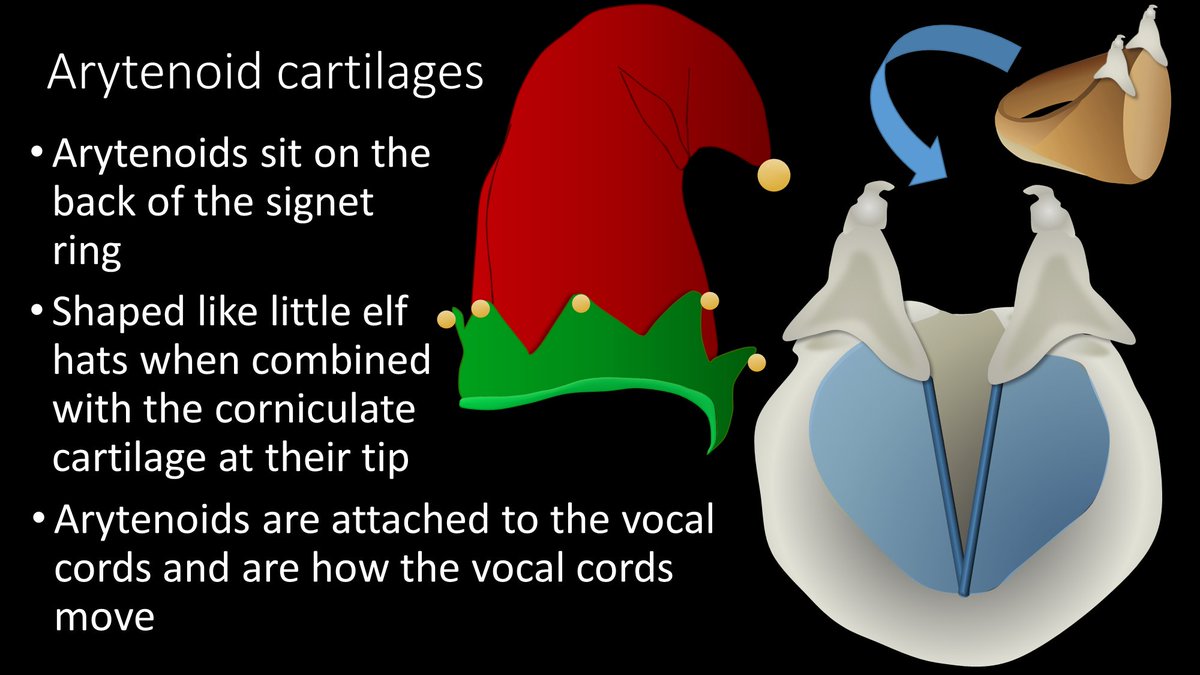
4/Arytenoid cartilages are these funny elf-hat shaped cartilages that are attached to the vocal cords. When the arytenoids move, your vocal cords move, and that's how phonation is created.
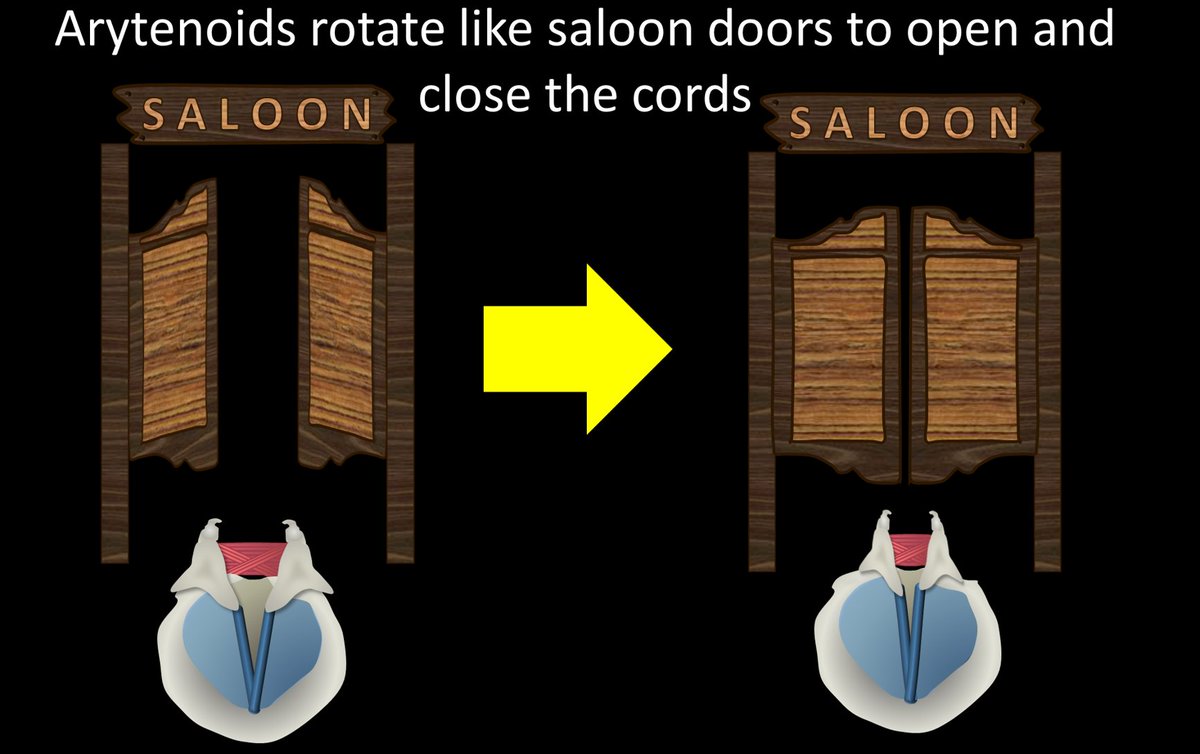
5/Arytenoids move by muscles that are stretched out between them, in a criss-cross pattern like shoe laces (transverse/oblique arytenoid muscles). When these muscles contract, it is like tightening shoe laces, which pull and rotate the arytenoids together
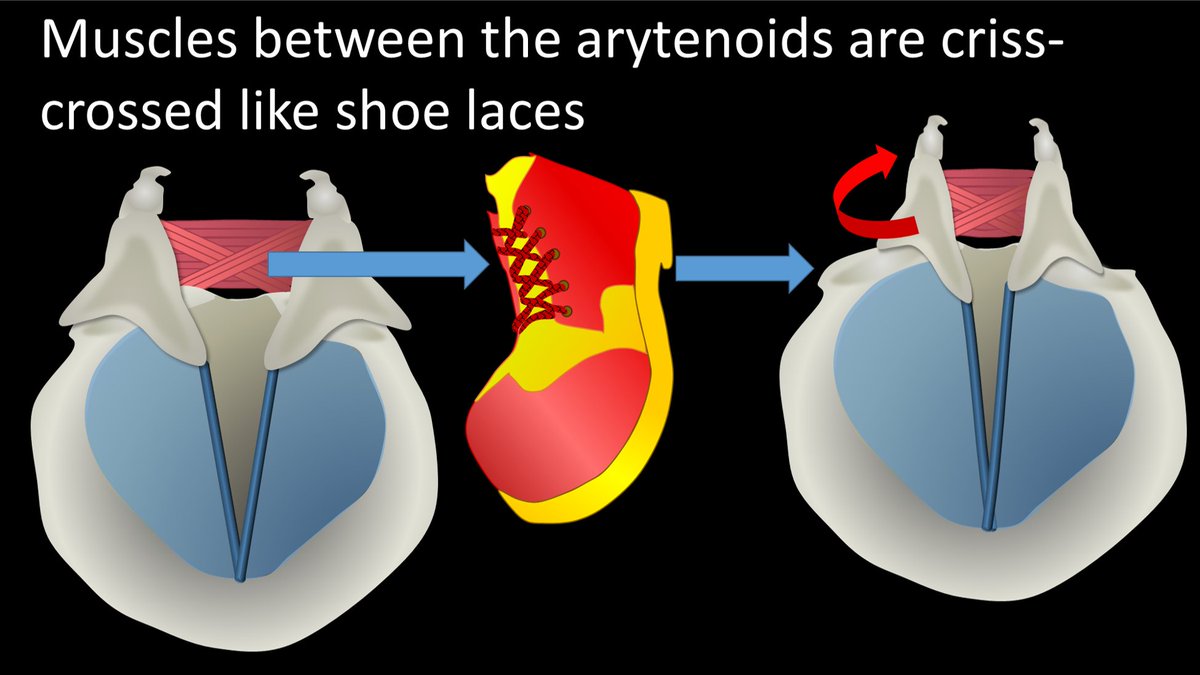
6/When the shoe laces are tightened or loosened, the arytenoids swing open or closed like an old fashioned saloon door--and open and close the vocal cords with them!
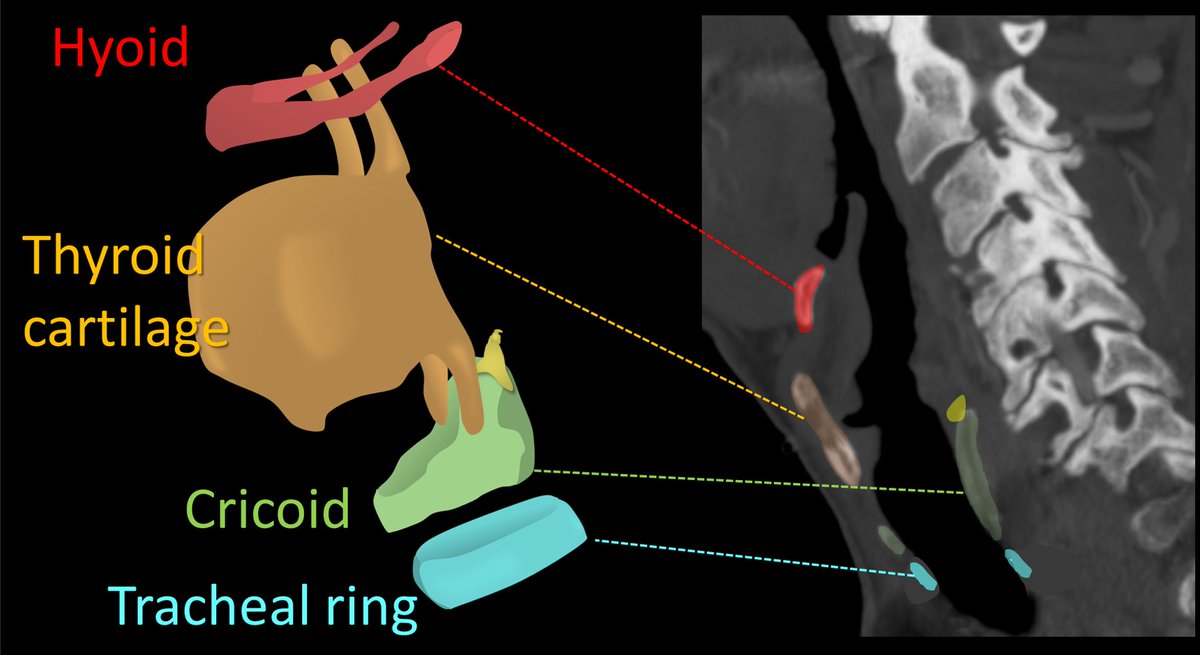
7/How the cricoid & arytenoids look on imaging depends on the level. Higher up, you are at the articulation of the arytenoids w/the signet ring & you see the crico-arytenoid joint. Lower down, you only see the posterior signet ring, & only at the bottom is entire ring visible

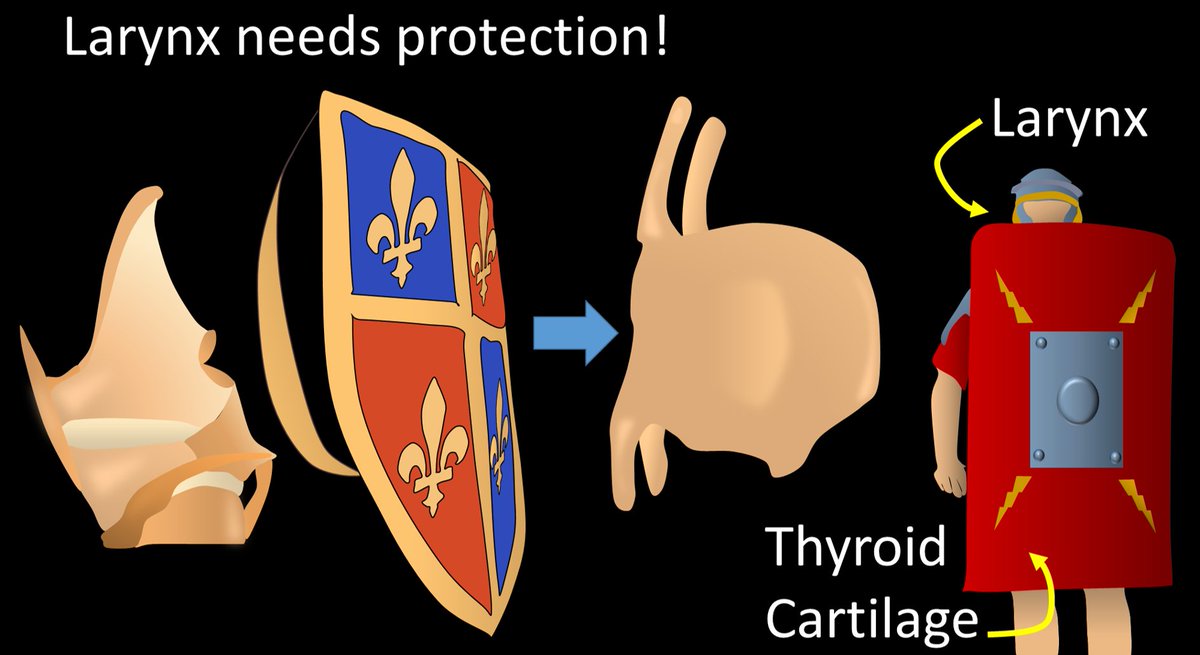
8/Larynx is so important to breathing & phonation that it needs protection--that is the thyroid cartilage. Thyroid cartilage is like a shield for the larynx. But it's huge, like those old Roman shields covering almost the entire body--that's the thyroid cartilage for the larynx
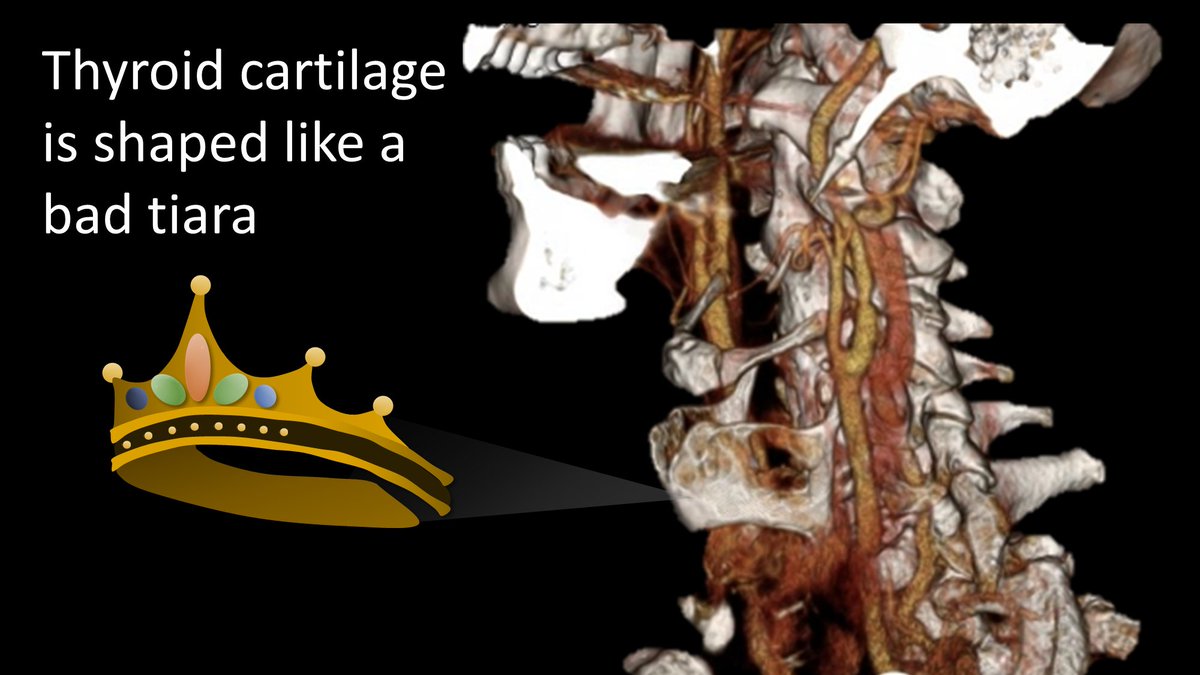
9/Thyroid cartilage is shaped like a bad tiara--except it has points going both up & down. It looks like one of those tiaras you thought would look great w/your prom dress at 16 &now you are stuck w/horrible photos where you look like a bad Disney princess--or was that just me?
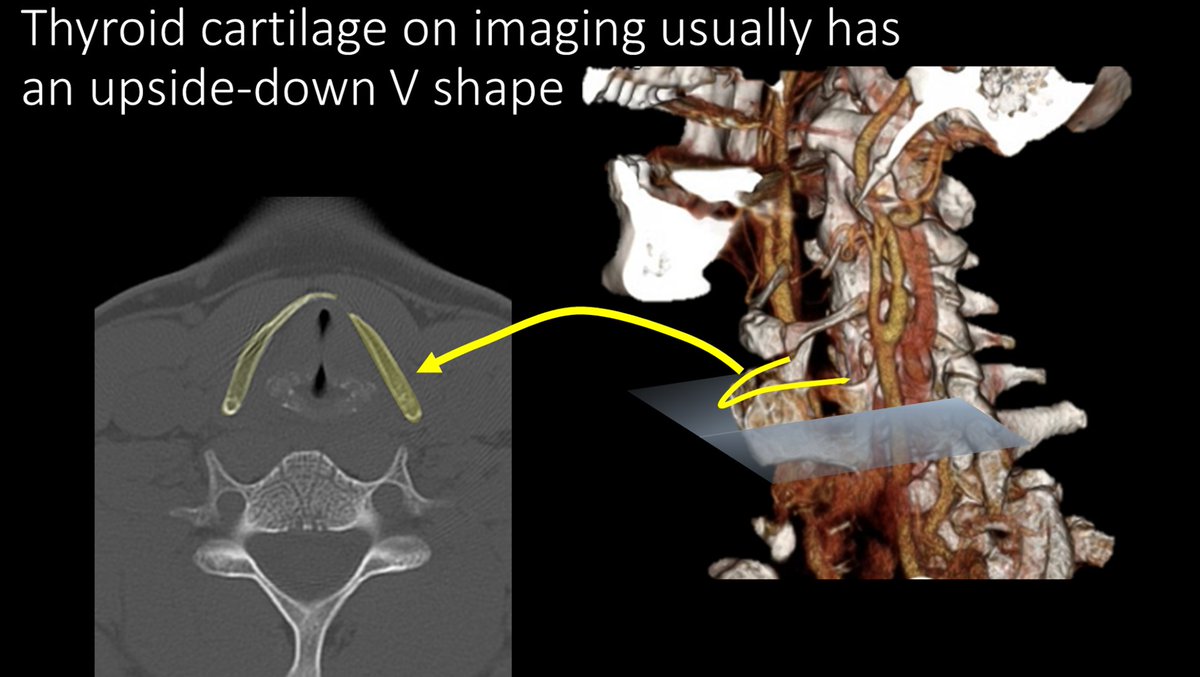
10/Because it is open posteriorly, like a tiara, and slightly pointed, on imaging--in cross section--it looks like a upside down letter V
11/So here's the summary of laryngeal supporting structures & how they relate to other structures. Hopefully this has shined some light on the black box of voice box anatomy!
Laryngeal anatomy is too complex for one tweetorial--this is just the beginning--stay tuned for more 😉
Laryngeal anatomy is too complex for one tweetorial--this is just the beginning--stay tuned for more 😉
• • •
Missing some Tweet in this thread? You can try to
force a refresh