Really important study being presented by Staci Gruber at #CPDD22 which longitudinally assesses a whole range of functioning in cannabis naive ppl before and following use of medical cannabis (now 3 years of follow up funded) 1/ 

2/ most interested in use for pain, detailed info collected on cannabinoid use..including developing the cannacount metric to measure cannabinoid use

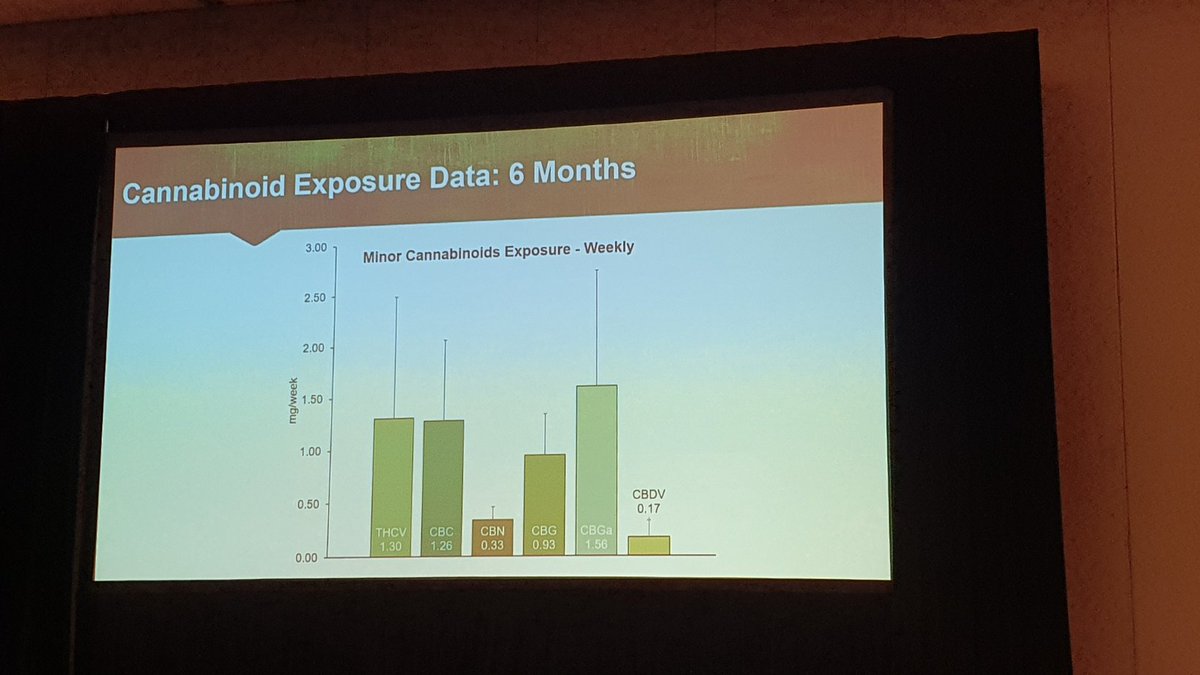
Most are using CBD dominant products, which include a range of other minor cannabinoids including CBG and CBC

Higher exposure to CBD appears to be associated with better mood related outcomes, and lower pain distress in the pain subset

• • •
Missing some Tweet in this thread? You can try to
force a refresh