
Let's be real. Whether you invoke the "with" vs "for" #Covid19 debate is besides the point. Hospital ERs weren't closing with this kind of regularity pre-pandemic. The burden of care has changed. Denying it will make things far worse. 1/
https://twitter.com/NightShiftMD/status/1543239983309398016
When patients either present with or acquire it in hospital, outcomes are often worse. As an internist, I see frail, elderly patients admitted w/ dehydration or a serious fall. They didn't just "happen" to have Covid too. It has actual implications. 2/
Just having to isolate a patient for infection control protocol means additional limitations for space/cohorting; greater demands on nursing care, infection control staff, never mind heightened risk & anxiety re: transmission for everyone. 3/
They might not die in hospital from Covid. But many decline directly as a result. Reduced respiratory reserve from scarred lungs, permanent organ dysfunction (need dialysis) or severe deconditioning happen, even with reinfection. 4/
This week I saw a handful of patients with Covid reinfection, some super sick. Not the picture of health to begin with but getting Covid heralded a dramatic decline I can't attribute to anything else. If I could I'd treat it. It's that simple. 5/
But the therapeutics are so much better now, right? Sort of. Steroids alone have no doubt saved a ton of lives but often that's not enough. Remdesivir is contraindicated in many whose kidney or liver function is abnormal (common in elderly/sick patients). 6/
What about Paxlovid? First there's a plethora of drug interactions, sometimes serious enough that using this would mean stopping another (essential) drug eg. some antipsychotics/cardiac drugs for 2 wks to give Paxlovid safely. Not a small ask. 7/
Add the increasing frequency of Paxlovid "rebound" infections due to emerging resistance mutations with BA.4 or BA.5 and suddenly this is anything but the silver bullet we had hoped for as our means to halt Covid reliably. (big sigh here) 8/
Remember monoclonal antibodies? Yeah, it seems like only yesterday they were incredibly effective life-savers. Omicron changed all of that. Sotrovimab? Regeneron? They're expensive placebos now. Useless. It didn't happen by accident. 9/
Let's imagine you don't even get admitted to hospital. You mask consistently, triple-vaxxed. But you've been exposed so often bc your kid brings it home from a class/daycare full of unmasked kids or staff. It's more than sniffles. It's way more. 10/
Your energy has vanished. Joints burn. Brain fog so bad you can't read directions on an instant soup without starting over a hundred times till you give up. Who are these people who have no daily dashboard or data post to acknowledge them? 11/
Many #LongCovid patients are health care workers. I see many w/no discernible risk factors for severe Covid (Diabetes/obesity/immune dysfn). But anyone can get Covid over & over if they are the only ones protecting themselves. They shouldn't have to. 12/
The divisiveness of the camps of alleged "fear-mongerers" vs "minimizers" is not helping. Hubris & disrespectful dialogue has done nothing but diminish the credibility, trust of PH messaging in the eyes of many. It's time to recalibrate. Now. 13/
We need data-driven opinions. We don't need any more opinion-driven opinions, esp if they might mean the difference between someone caring or not caring about a virus that continues to evolve. Your opinion could squander lives as easily as saving one. 14/
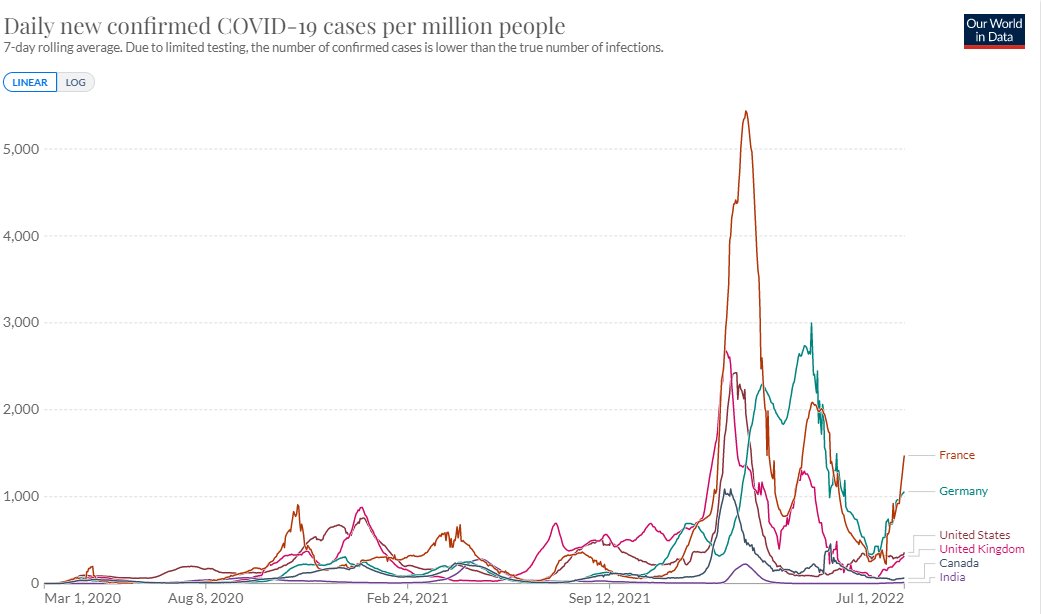
If you're confident enough that the surge in UK hospitalizations from BA.5 won't be on our doorsteps in Canada/US in a few weeks, I want to ask what this is based on. Every single wave here was previewed ~ 6 wks before in UK. What changed...? 15/ 
The dismissiveness of masking as the most basic & visible symbol of awareness that this virus is still here & capable of real harm is a cardinal misstep. The minimizing of vaccination benefit is equally troubling. The message has become lost. 16/
Too many people believe this is over & look for anyone to help validate this whether by Twitter/TV/other following. The more you hear it, the better it sounds, the easier you go on #LivingWithCovid. Until maybe you actually have to Live. With. Covid. 17/
And who will care for you, your friend, your loved one in the ER/ICU when RNs, MDs, RTs, PTs, OTs, social workers, other HC staff have quit, burned out, on long-term leave? It's already happening. It will get far worse if we pretend otherwise. #WeNotMe 18/
So I'll end with this. Stop looking for a "one & done" answer for the most challenging virus we've faced in over a century. The solution is not ONLY vaccines/masking/ventilation but ALL of them. More is better. Health that is. Not virus. 19/fin
• • •
Missing some Tweet in this thread? You can try to
force a refresh


