
How we used to identify monoclonal proteins (electrophoresis, immunofixation, left).
How we identify monoclonal proteins now @MayoClinic (mass spectrometry, right).
#myeloma #MGUS #MedTwitter
How we identify monoclonal proteins now @MayoClinic (mass spectrometry, right).
#myeloma #MGUS #MedTwitter


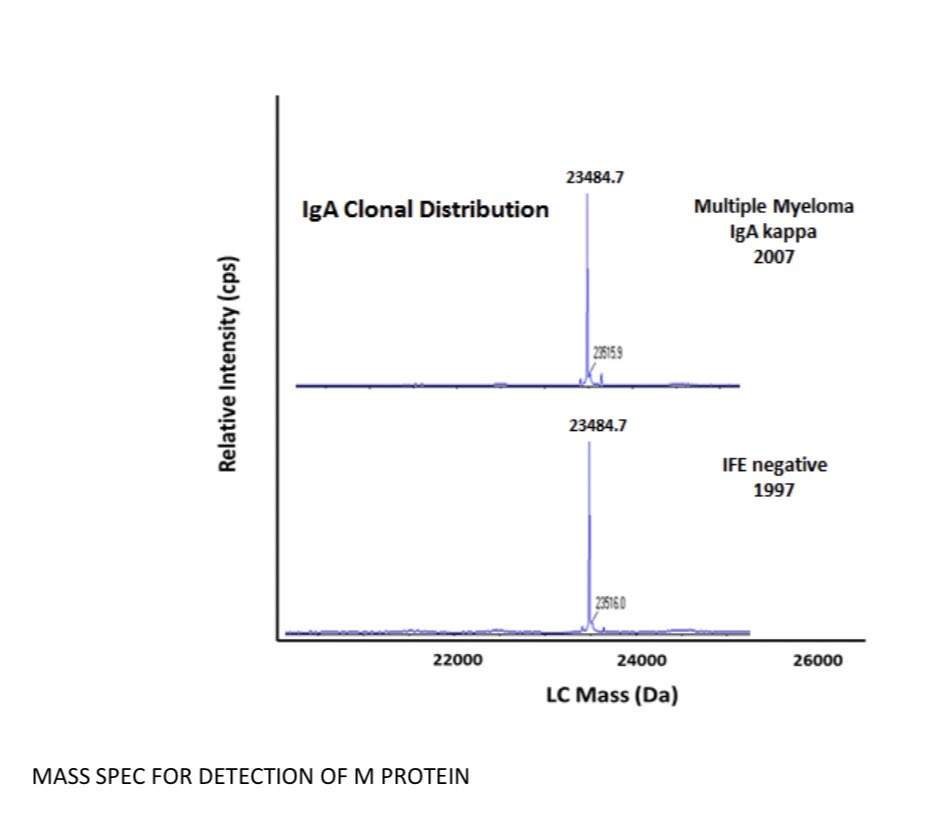
Patient with IgA monoclonal protein with molecular weight of 23484.7 diagnosed in 2007.
Same patient had same monoclonal protein 10 years ago that was not detected by immunofixation, but we could readily detect on mass spec done on archival serum sample.
Same patient had same monoclonal protein 10 years ago that was not detected by immunofixation, but we could readily detect on mass spec done on archival serum sample.
Mass spec is more accurate, easier and more efficient for labs. @moricemdphd
Using clinical grade mass spectrometry, we estimate 5% of the general population age 50 and older has a monoclonal protein, (MGUS).
Our prior estimate with electrophoresis and immunofixation was 3%. @BloodCancerJnl @MayoMyeloma nature.com/articles/s4140…
Our prior estimate with electrophoresis and immunofixation was 3%. @BloodCancerJnl @MayoMyeloma nature.com/articles/s4140…
Mass spec needs expertise in set up and interpretation. If you don't know what you are doing, you can find a "monoclonal protein" in everyone.
So we have to set the right thresholds for proper clinical use.
So we have to set the right thresholds for proper clinical use.
• • •
Missing some Tweet in this thread? You can try to
force a refresh



