There are ~10 million doctors in the world.
Here are 10 who have literally been 1 in a million during the pandemic.
We can't thank you enough. 🙏
Here are 10 who have literally been 1 in a million during the pandemic.
We can't thank you enough. 🙏










There are many, many others who have contributed as well.
Thank you to all. 🙏
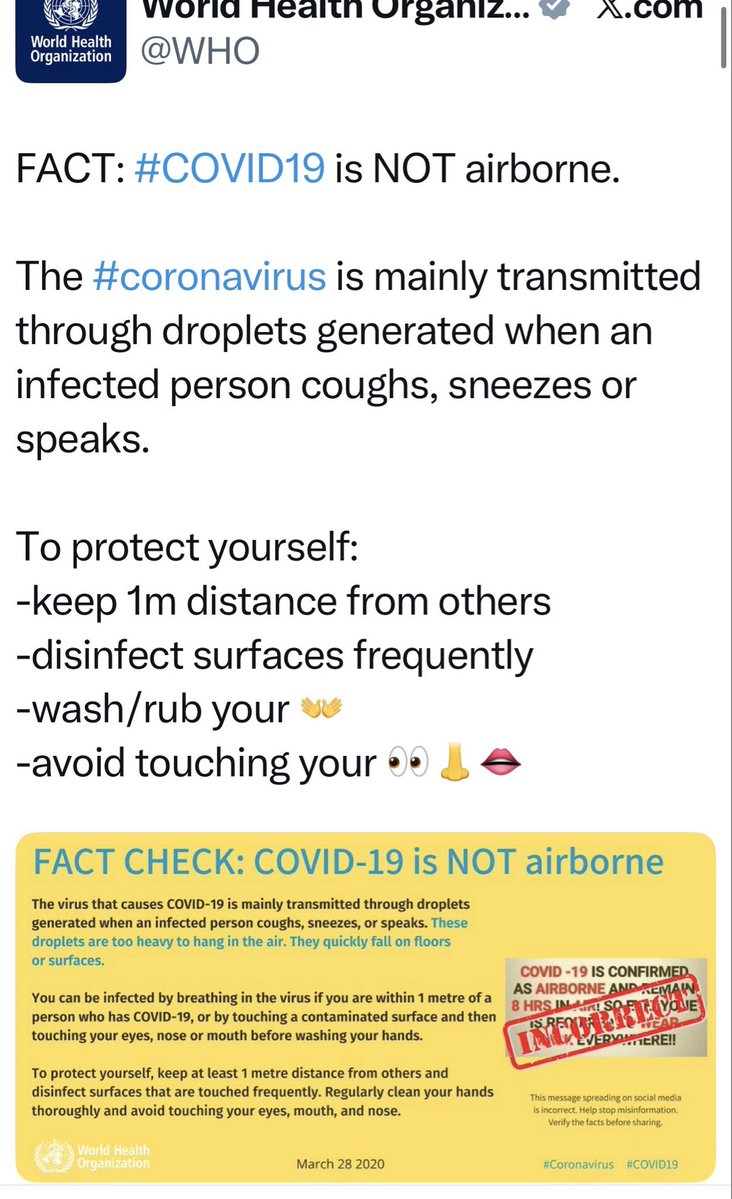
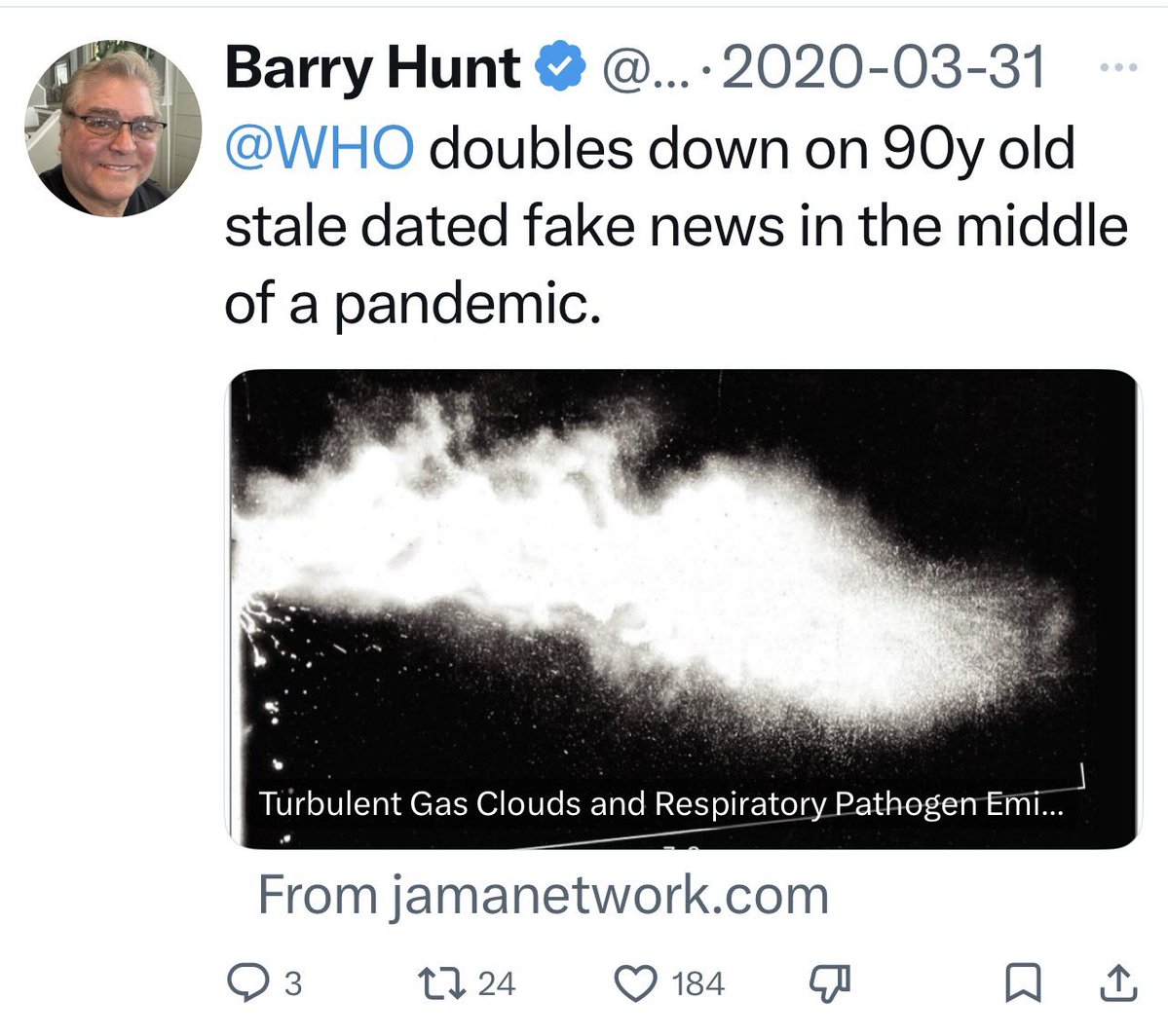
#COVIDisAirborne
#CovidIsNotOver
#MonkeyPoxIsAirborne
Thank you to all. 🙏
#COVIDisAirborne
#CovidIsNotOver
#MonkeyPoxIsAirborne
• • •
Missing some Tweet in this thread? You can try to
force a refresh