Pt seen in ambulatory clinic with worsening kidney function
While the patient is sitting down (90 degrees), you notice neck pulsations!
Are they arterial or venous??
1/4 🧵
While the patient is sitting down (90 degrees), you notice neck pulsations!
Are they arterial or venous??
1/4 🧵
It is single peak (but not sharp)
The most striking feature is the inward movement
The breath of movement is diffuse
These are signs of venous pulsations!
Very helpful table from @AndreMansoor 👇
2/4
The most striking feature is the inward movement
The breath of movement is diffuse
These are signs of venous pulsations!
Very helpful table from @AndreMansoor 👇
2/4

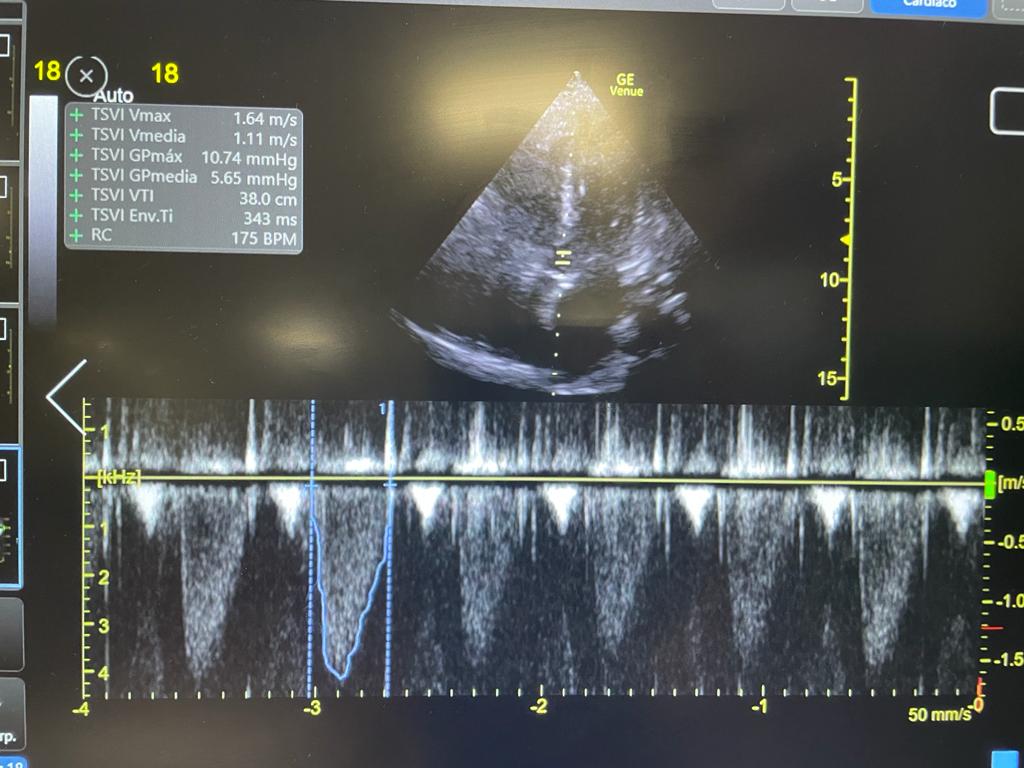
Thankfully we have #POCUS in clinic! I believe #POCUS can really help you improve your classic physical exam skills as it gives you immediate feedback!
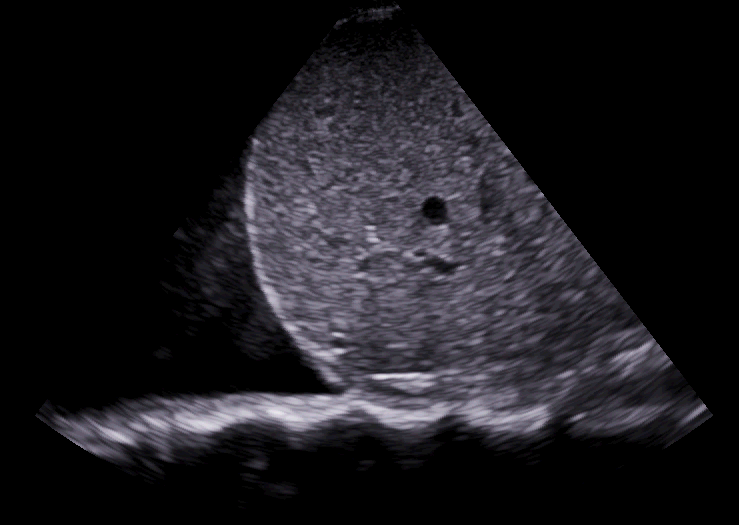
Quick #VExUS reveals plethoric IVC, reverse S wave on Hepatic Vein, >100% portal vein pulsatility and mono-phasic IRVD!
3/4
Quick #VExUS reveals plethoric IVC, reverse S wave on Hepatic Vein, >100% portal vein pulsatility and mono-phasic IRVD!
3/4




This patient has severe TR with severe congestion. This explains why JV waveform has a single peak rather than double (CV fusion 2/2 TR)
#POCUS is no replacement for physical exam, but it certainly enhances it! #VExUS gives you quantitative data as well!
/END
#POCUS is no replacement for physical exam, but it certainly enhances it! #VExUS gives you quantitative data as well!
/END
• • •
Missing some Tweet in this thread? You can try to
force a refresh