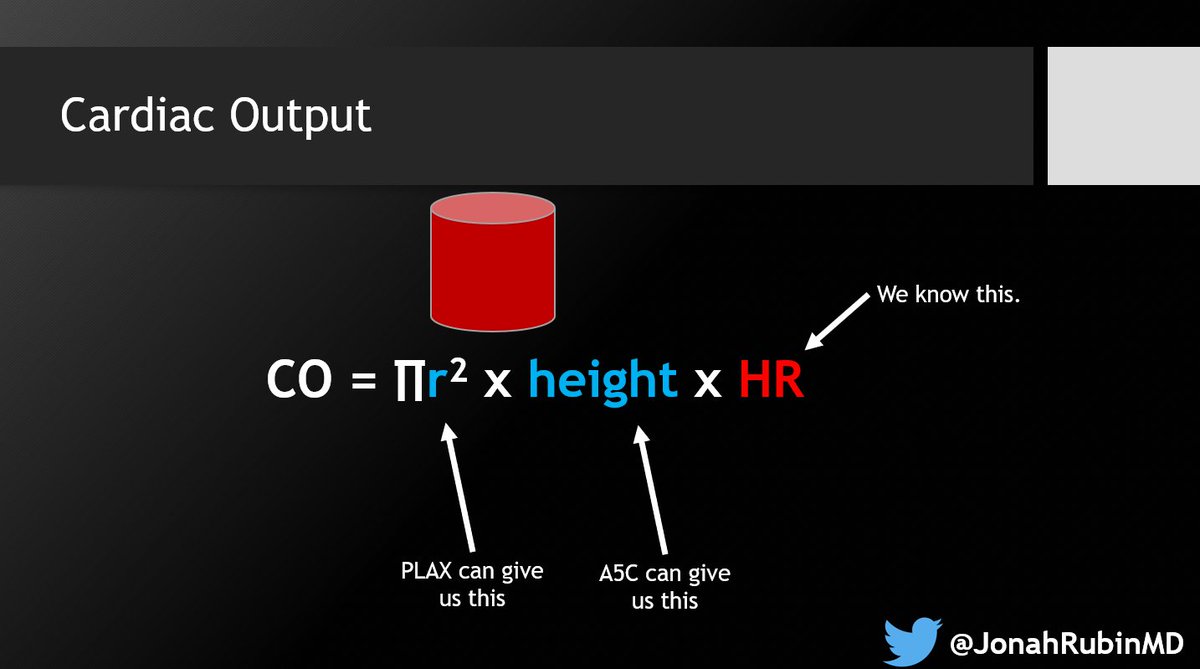
Cardiac Output by VTI!
Summary slides from our next lecture, broken into 5 steps⤵️
@MGH_PCCM @HarvardPulm @MGHHCICU
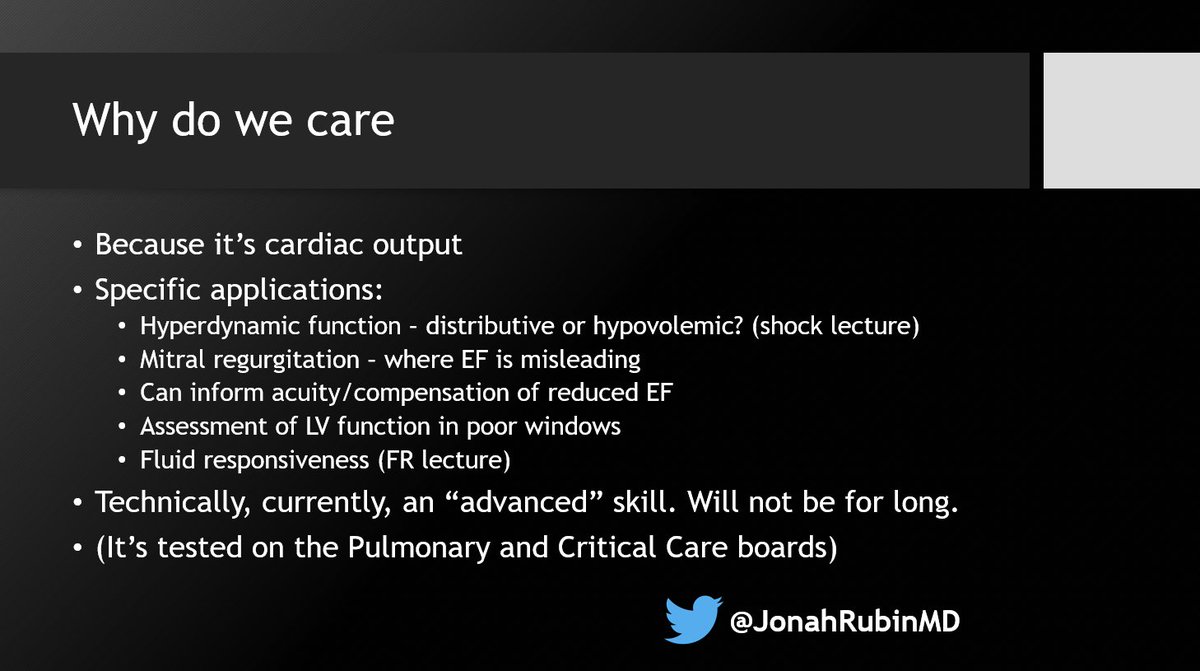
1⃣ Overview & approach - and why you care. CO adds significant detail and nuance to LV function assessment
#POCUS #Medtwitter #PCCMtwitter #echofirst
Summary slides from our next lecture, broken into 5 steps⤵️
@MGH_PCCM @HarvardPulm @MGHHCICU
1⃣ Overview & approach - and why you care. CO adds significant detail and nuance to LV function assessment
#POCUS #Medtwitter #PCCMtwitter #echofirst


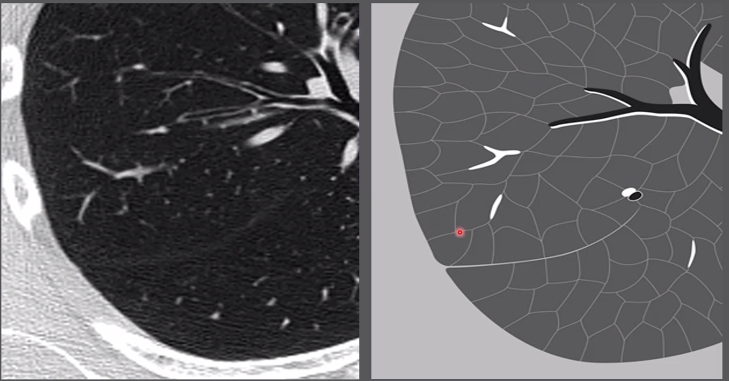
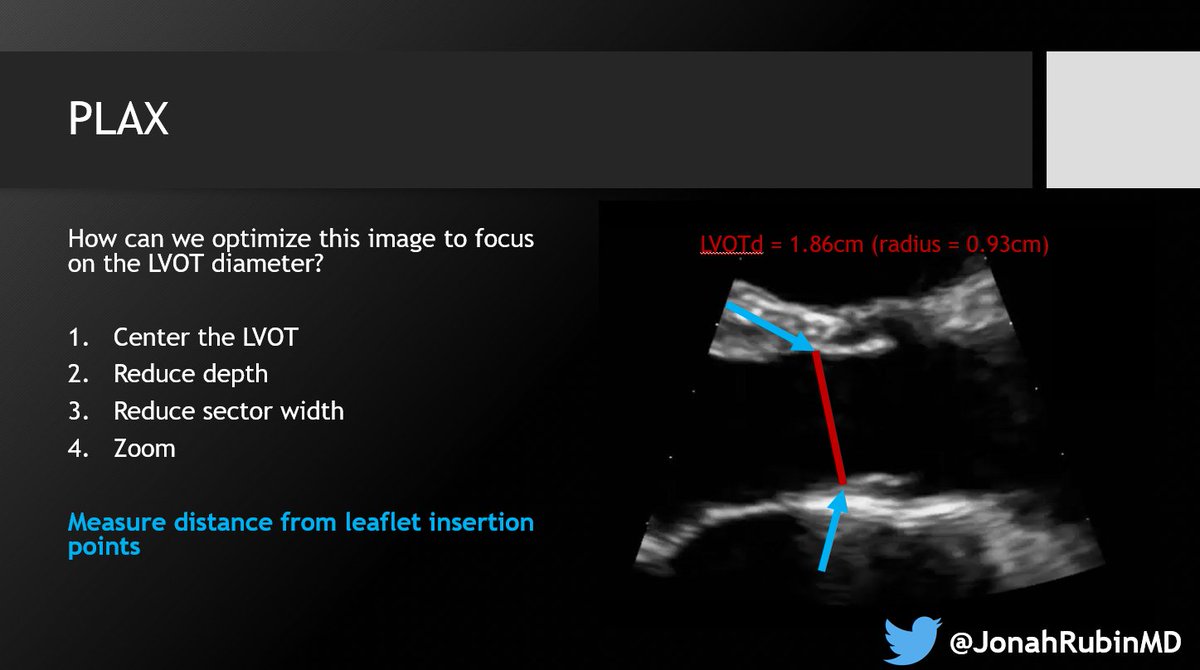
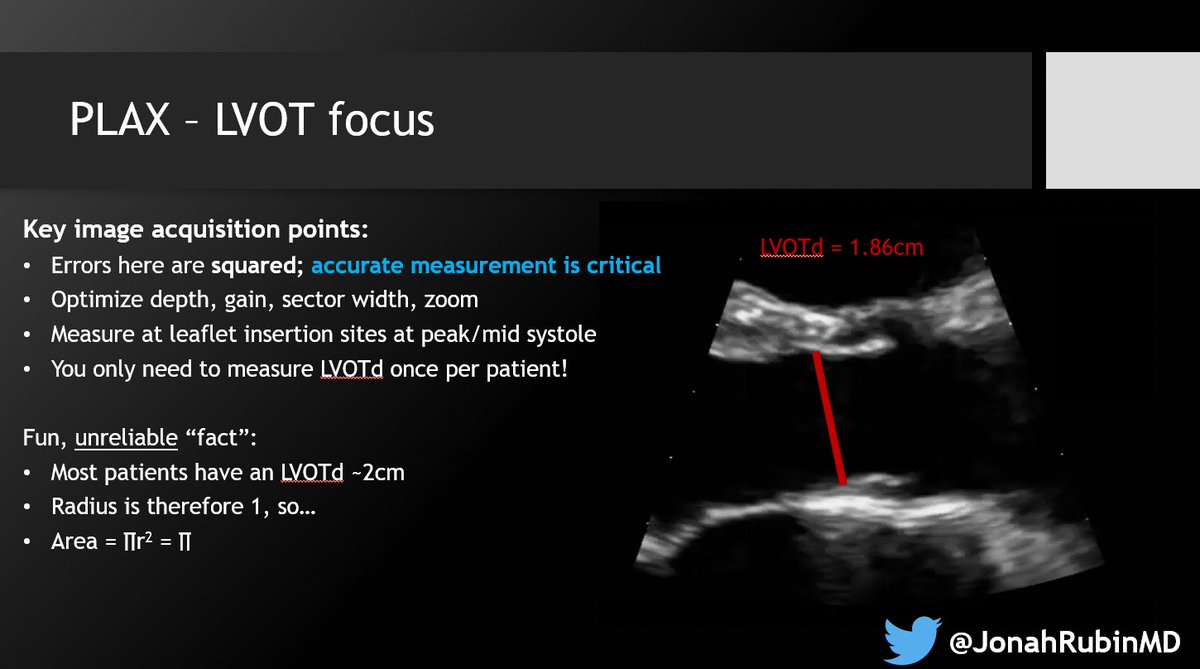
2⃣ Optimize the PLAX for the LVOTd. Sometimes I find that too much "optimization" actually makes it harder. Just know your options and do what works with your patient.
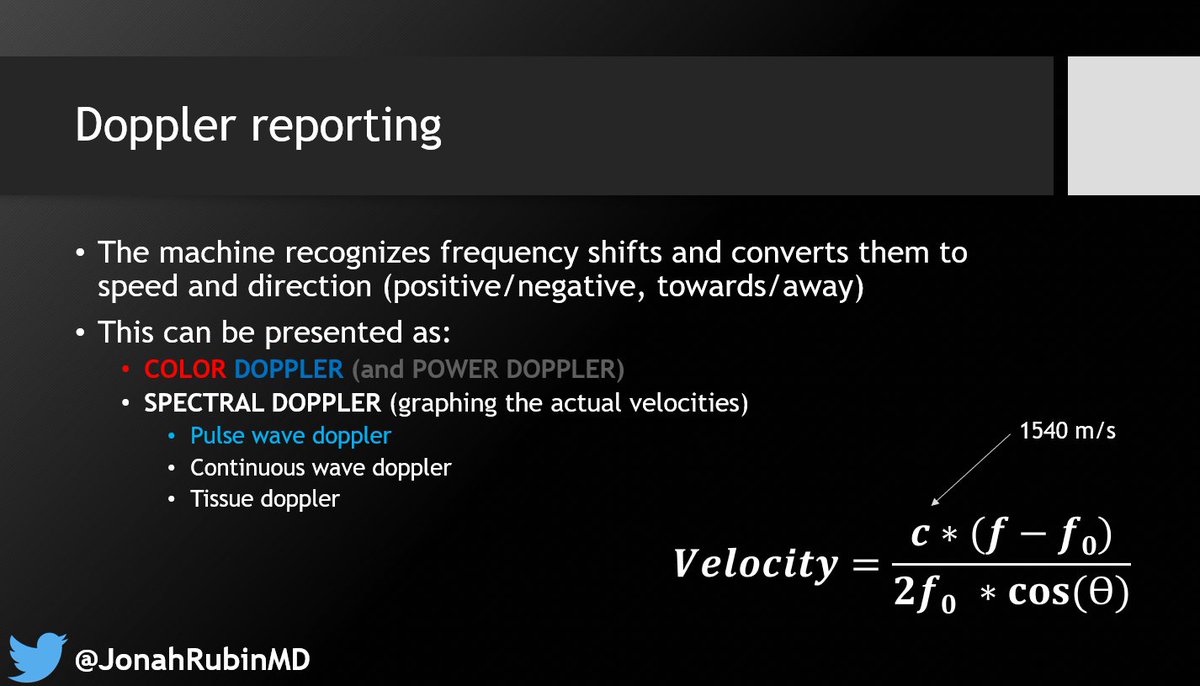
3⃣ Understand Doppler physics. Specifically PWD for this one. Recognize how the angle of insonation AND the angle of flow relative to the probe, affects your measurements.
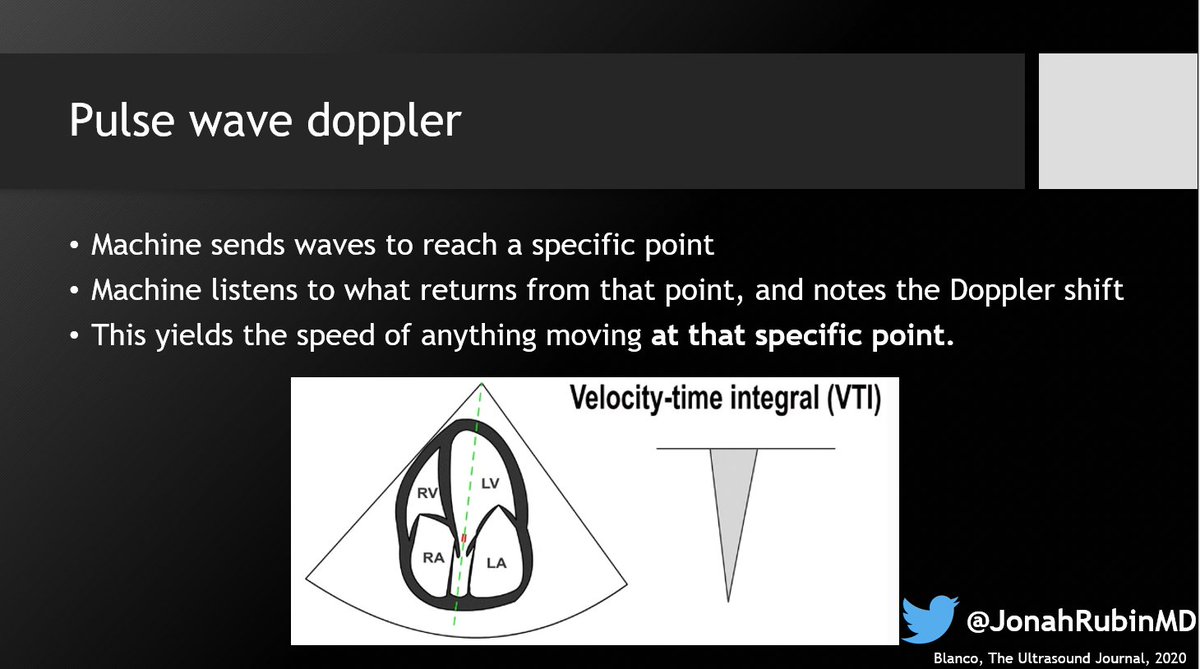
4⃣ Get that VTI - properly! Angle adjustments are eh. At best they correct for one dimension, and not really for your angle of insonation. Not ideal, but if you must.

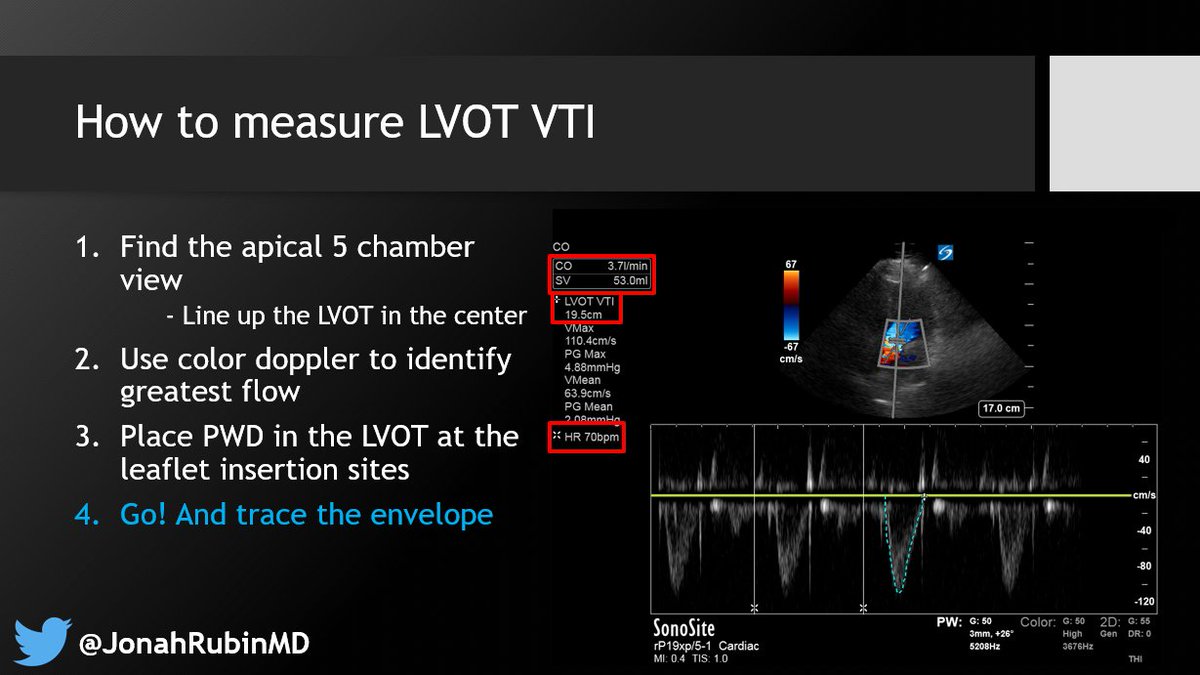

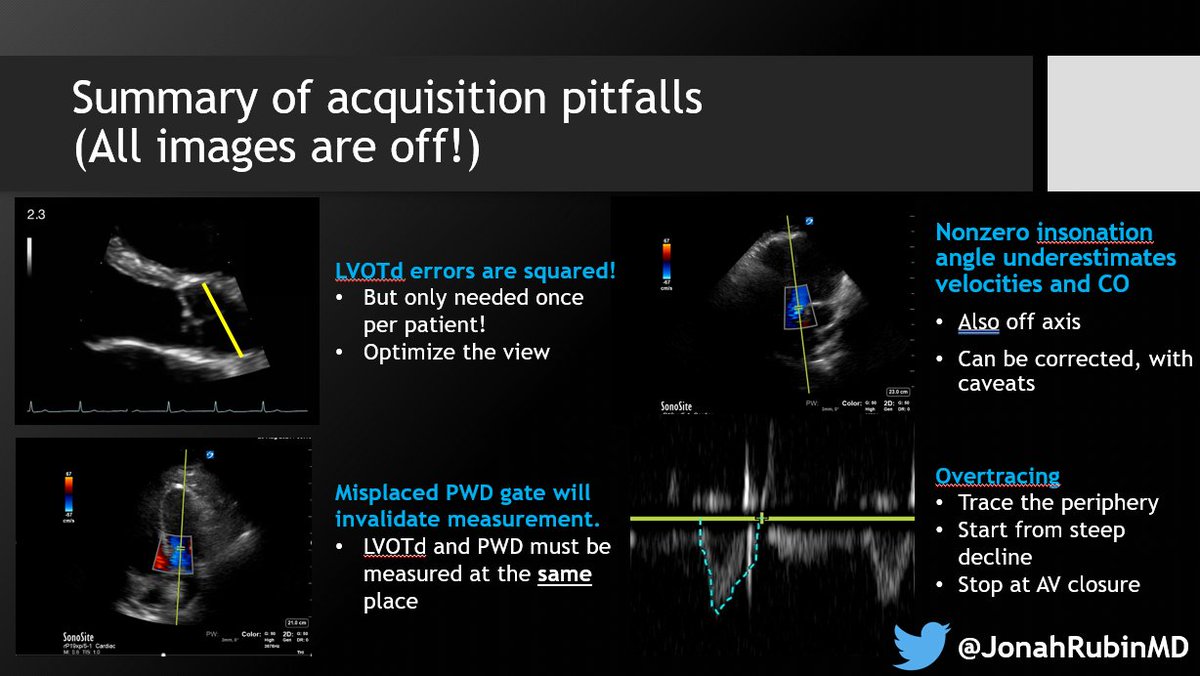
5⃣ Finally - mind the pitfalls, in both acquisition & interpretation. Being off angle can only underestimate VTI, but overtracing can overestimate.
Anything else you'd like to see or add? Comments always welcome!
@katiewiskar @echonepean @khaycock2 @ThinkingCC @EchoSoliman @siddharth_dugar @Thind888 @ThinkingCC @icmteaching @ria_dancel @POCUSEcho @msiuba @MaxHockstein @cameron_baston @Yonatan_G_MD @nickmmark @NephroP @avkwong @POCUSEcho @critconcepts @iceman_ex @kyliebaker888 @MRamzyDO
If you're interested in having this lecture delivered at your institution, DMs are open - happy to discuss!
• • •
Missing some Tweet in this thread? You can try to
force a refresh