SEIZURE SEMIOLOGY TWEETORIAL
#Epilepsy #Neurotwitter #Seizure #Semiology
🧵1/ What is a somatosensory aura?
A somatosensory aura is an abnormal subjective somatic sensation, involving one or more body parts, typically described as 'tingling' or 'numbness'.
#Epilepsy #Neurotwitter #Seizure #Semiology
🧵1/ What is a somatosensory aura?
A somatosensory aura is an abnormal subjective somatic sensation, involving one or more body parts, typically described as 'tingling' or 'numbness'.


2/ There are three main types of somatosensory auras: Paresthetic auras, Painful auras, Thermal auras
Paresthetic auras are probably the most common type reported by patients.
Paresthetic auras are probably the most common type reported by patients.


3/ Paresthetic auras are reported by patients as tingling, numbness or both. These often occur in discrete body parts such as fingers, hand, face etc. and are mostly lateralized. Just like focal clonic seizures, these auras can show a "Jacksonian march".



4/ In one of the largest series ever published on somatosensory auras, the most common sites of these auras were hand & fingers, feet and face.


5/ The symptomatogenic zone of the paresthetic auras is most likely area SI or the primary somatosensory cortex, located in the post-central gyrus (Brodmann area 3b mainly, 1 and 2)



6/ The paresthetic or SI auras, when restricted to limbs, are almost exclusively contralateral. The S1 aura of the face can be bilateral or contralateral but almost never ipsilateral.


7/ The somatotopic map of the SI is well established and it is almost the same as the Penfield motor homunculus.

8/ The other symptomatogenic zone of paresthetic auras is SII or second sensory area, located in the parietal opercular cortex, with it's own distinct homunculus. The presence of this area in cats was first reported by Adrian and Woolsey in the 1940s.



9/ The presence of SII area in humans was first reported by Penfield in 1947 and further elaborated by Penfield and Rasmussen in 1950.



10/ Mazzola, et al. demonstrated that majority of SII stimulations produced paresthetic auras, followed by thermal auras being the second most common. But the SII paresthetic auras are not as discrete as SI auras and the somatotopic organization doesn't follow SI homunculus.




10/ Just like SI, majority of SII limb paresthetic auras are contralateral, but can be bilateral or ipsilateral.

11/ The somatotopic map of SII is relatively well established now since Penfield's original work and has been studied by many investigators. The homunculus is circumscribed and is very condensed. Hand is rostral to face.


12/ Painful and thermal auras are probably the rarest of somatosensory auras. In Penfield & Kristiansen, out of 55 cases with somatosensory auras, only two described these as "cramp-like" pain and four patients described a "thermal" sensation.

13/ In Mauguiere and Courjon's series, pain was the second most common type of somatosensory aura, followed by temperature.

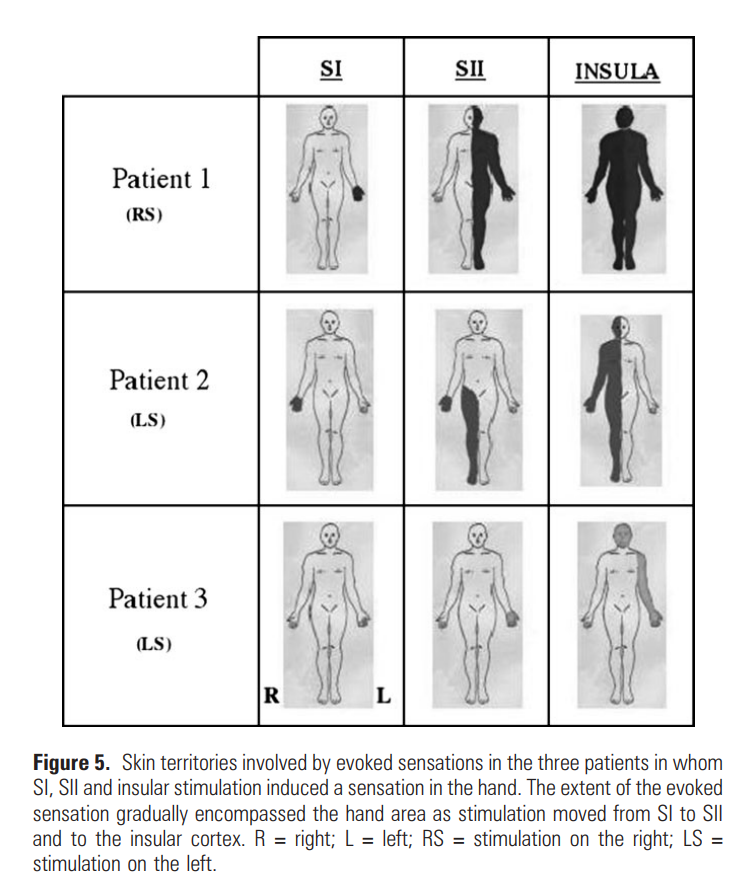
14/ The most likely symptomatogenic zone for painful and thermal auras is the insula or SIII. Majority of stimulation studies have been able to elicit sensations from posterior insula, behind the central sulcus.
15/ Within the posterior insula, from anterior to posterior are- primary & secondary gustatory area, viscerosensitive area, thermal and nociception and general tertiary somatosensory area. @guadalupefbv


16/ Most commonly elicited aura from insular stimulation is still paresthetic, followed by thermal and painful. Most limb sensations are contralateral like SI and SII, but a large percentage of face and trunk sensations are bilateral.


17/ The most common epileptogenic zone associated with somatosensory auras is parietal or peri-rolandic.


18/ SSMA stimulations are also known to produce sensations but these are often bilateral, poorly described and poorly localized.
19/ Conclusions: Most common somatosensory auras are paresthetic, followed by pain and temperature. SI auras are mostly contralateral with discrete localization. SII auras are more widespread and can be bilateral or ipsilateral, but mostly contralateral in limbs.
20/ SIII or insular auras are more likely to be pain and temperature related than SI and SII. The limb SIII auras are mostly contralateral but face and trunk are mostly bilateral and can be ipsilateral. #neurotwitter #epilepsy #seizure #semiology
• • •
Missing some Tweet in this thread? You can try to
force a refresh