Day 2 PM session : Advanced monitoring in acute Resp failure. Opening on #NIV Non invasive support - Domenico and Oriol Rica. #LIVES2022
#ventilation
ARF: NIV evidence clear In acute cariogenic pulmonary oedema / hypercapnia ARF. not so clear in hypoxemic ARF
#ventilation
ARF: NIV evidence clear In acute cariogenic pulmonary oedema / hypercapnia ARF. not so clear in hypoxemic ARF
starting with a case : 55,male,no PMH. SOB in 2/days, fever 1/ week. PaO2 11(90), 10 l o2 facemask, PaCO2 3.7 (28), pH 7.48, lac 1.5, RR 33, BP 140/70, HR 130bpm sinus. CXR: four quadrant consolidate changes. Immediate thoughts?
Q. what's the estimate of FiO2? 3% formula FiO2 fairly good estimate.
pubmed.ncbi.nlm.nih.gov/32522764/
pubmed.ncbi.nlm.nih.gov/32522764/
Clinically how is he? 5 out of 10 dyspnoea. (NOTE: not a covid patient).
What would you do next? a). NIV b). cPAP c). High Flow Nasal Cannulae(HfNC)
Be mindful of delay in intubation : see this study
pubmed.ncbi.nlm.nih.gov/22318634/
What would you do next? a). NIV b). cPAP c). High Flow Nasal Cannulae(HfNC)
Be mindful of delay in intubation : see this study
pubmed.ncbi.nlm.nih.gov/22318634/
Don’t forget the hidden part of Pmusc. Think transpulmonary pressure which is what contributed to lung injury. 
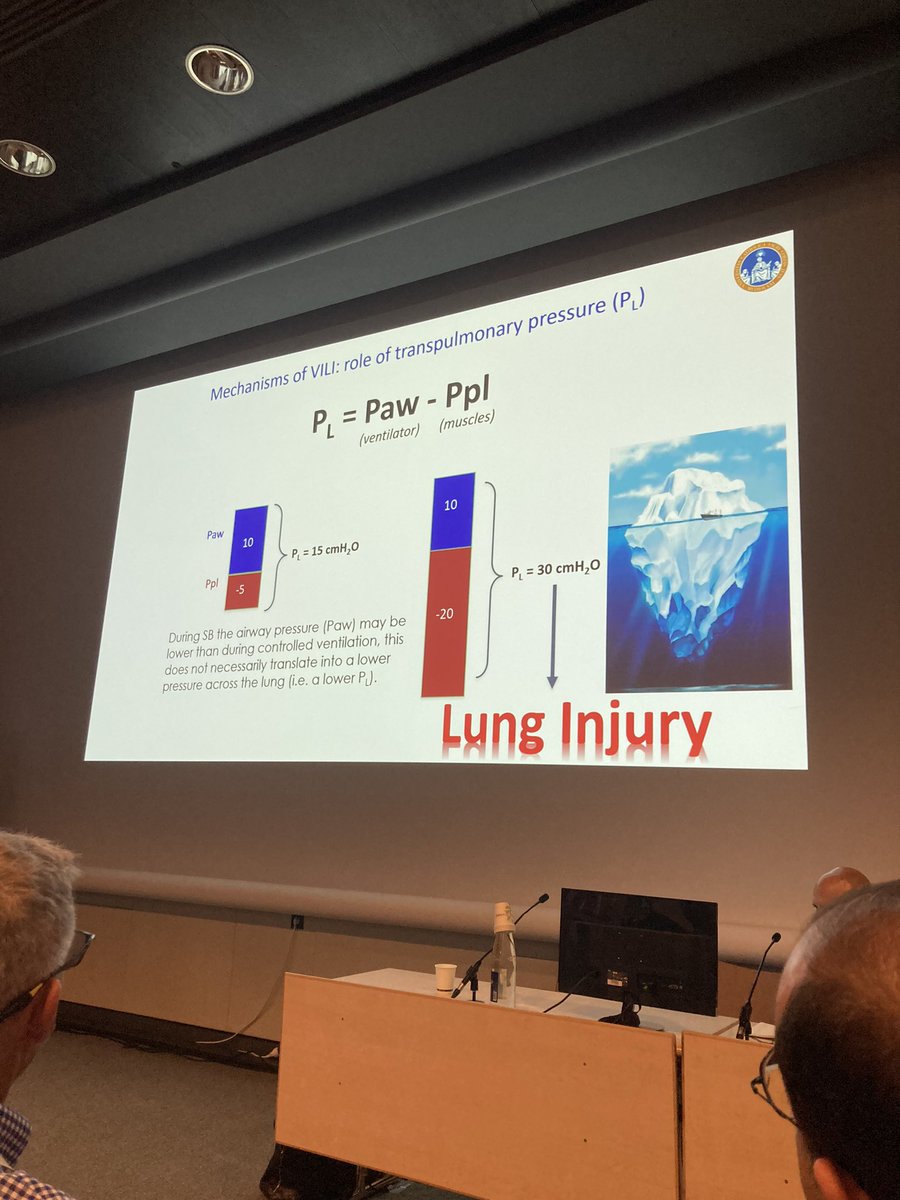
Has effect on haemodynamics so can worsen oedema

can have occult pendelluft. best work :atsjournals.org/doi/full/10.11… pubmed.ncbi.nlm.nih.gov/24199628/
pubmed.ncbi.nlm.nih.gov/27997805/
pubmed.ncbi.nlm.nih.gov/27753501
high flow >> conventional o2. easier to breathe and patient satisfaction
pubmed.ncbi.nlm.nih.gov/27753501
high flow >> conventional o2. easier to breathe and patient satisfaction
IDEALLY, WHAT would you monitor during treatment?
1. spo2/fio2 2. RR 3. Dyspnoea 4. PaO2/FiO2 5. Inspiratory Effort
Ideally all of them but if have to pick 2, which would you pick?
1. spo2/fio2 2. RR 3. Dyspnoea 4. PaO2/FiO2 5. Inspiratory Effort
Ideally all of them but if have to pick 2, which would you pick?
pubmed.ncbi.nlm.nih.gov/30576221/
The original ROX score. ROX = (SpO2/FiO2) / (Resp Rate)
ROX <2.85, <3.47 and <3.85 at 2,6 and 12 hr predictors of HFNC failure. SpO2/FiO2 have higher weight than RR
The original ROX score. ROX = (SpO2/FiO2) / (Resp Rate)
ROX <2.85, <3.47 and <3.85 at 2,6 and 12 hr predictors of HFNC failure. SpO2/FiO2 have higher weight than RR
the graph hidden in that paper is also Relative Risk of death in hospital for delayed patients. potentially higher. ROX validation in COVID patient. In COVID 19 ,RR tend to be higher. But validated
pubmed.ncbi.nlm.nih.gov/32671470/
pubmed.ncbi.nlm.nih.gov/32671470/
love this paper : ncbi.nlm.nih.gov/pmc/articles/P…
The more time the patient spend on sport breathing with hypoxemia, more time in higher driving pressure. same with RR > 25. No Resp effort in this paper but if there is Resp effort, it will be even stronger.
The more time the patient spend on sport breathing with hypoxemia, more time in higher driving pressure. same with RR > 25. No Resp effort in this paper but if there is Resp effort, it will be even stronger.

so the holy grail : lets measure inspiratory effort with oesophageal balloon for NIV.
pubmed.ncbi.nlm.nih.gov/32325004/
pubmed.ncbi.nlm.nih.gov/32325004/
THE harm of spontaneous breathing -- real. and the only real way of measuring it is via Oesophageal catheter. Great graphics (where if your inspiratory effort does not improve with NIV -- failure).
Q1: pharmacological Rx to augment p-SILI ? dexmedetomidine shouldn't affect Resp drive but if it helps calm the patient may have a role. opioids - reduce rate but not necessarily effort. Q2:: effort vs. RR? Ans:EFFORT is more important as early adaptation RR is late adaptation.
PEOPLE WITHOUT OESOPHAGEAL PRESSURE -- what can you do? CVP line -- CVP big swing of intra-thoracic pressure. But for this purpose only, why would you want to CVP which is more invasive than oesophageal catheter.
Q3. cPAP vs. NIV. Again the unifying theme would be "patient's own inspiratory effort". Future is in "patient's own inspiratory effort" -- this is a denominator that helps decide cPAP vs. HfNC vs. NIV vs. Intubation.
• • •
Missing some Tweet in this thread? You can try to
force a refresh