1/ 🚨 #5Pearls on Alcohol-Associated Hepatitis 🚨
Why is it an immune response?
✔️Direct EtOH insult ➡️ inflammation
✔️Disruption of the gut barrier ➡️ bacteria & inflammatory cells go up portal vein ➡️ to hepatocytes
🎧 link.chtbl.com/AlcHep
Sponsor: @Pan_Financial
Why is it an immune response?
✔️Direct EtOH insult ➡️ inflammation
✔️Disruption of the gut barrier ➡️ bacteria & inflammatory cells go up portal vein ➡️ to hepatocytes
🎧 link.chtbl.com/AlcHep
Sponsor: @Pan_Financial

2/ Now, What else may be going on & what imaging and labs would you send off for ddx for Alc Hep?
Listen to the episode to hear a powerful story from @etapper differentiating Alc hep and worsening #cirrhosis
Listen to the episode to hear a powerful story from @etapper differentiating Alc hep and worsening #cirrhosis

3/ What interventions are most linked to improved mortality?
Alcohol cessation and nutrition!
Alcohol leads to⬇️absorption of proteins, carbs, and fats as well as impaired absorption of micronutrients = Alc Hep induces catabolic state
See some tips below for daily targets!
Alcohol cessation and nutrition!
Alcohol leads to⬇️absorption of proteins, carbs, and fats as well as impaired absorption of micronutrients = Alc Hep induces catabolic state
See some tips below for daily targets!

4/ Abstinence of alcohol after episode of alcohol associated hepatitis positively impacts long term survival📈;⬇️ risk of mortality by close to 50% !
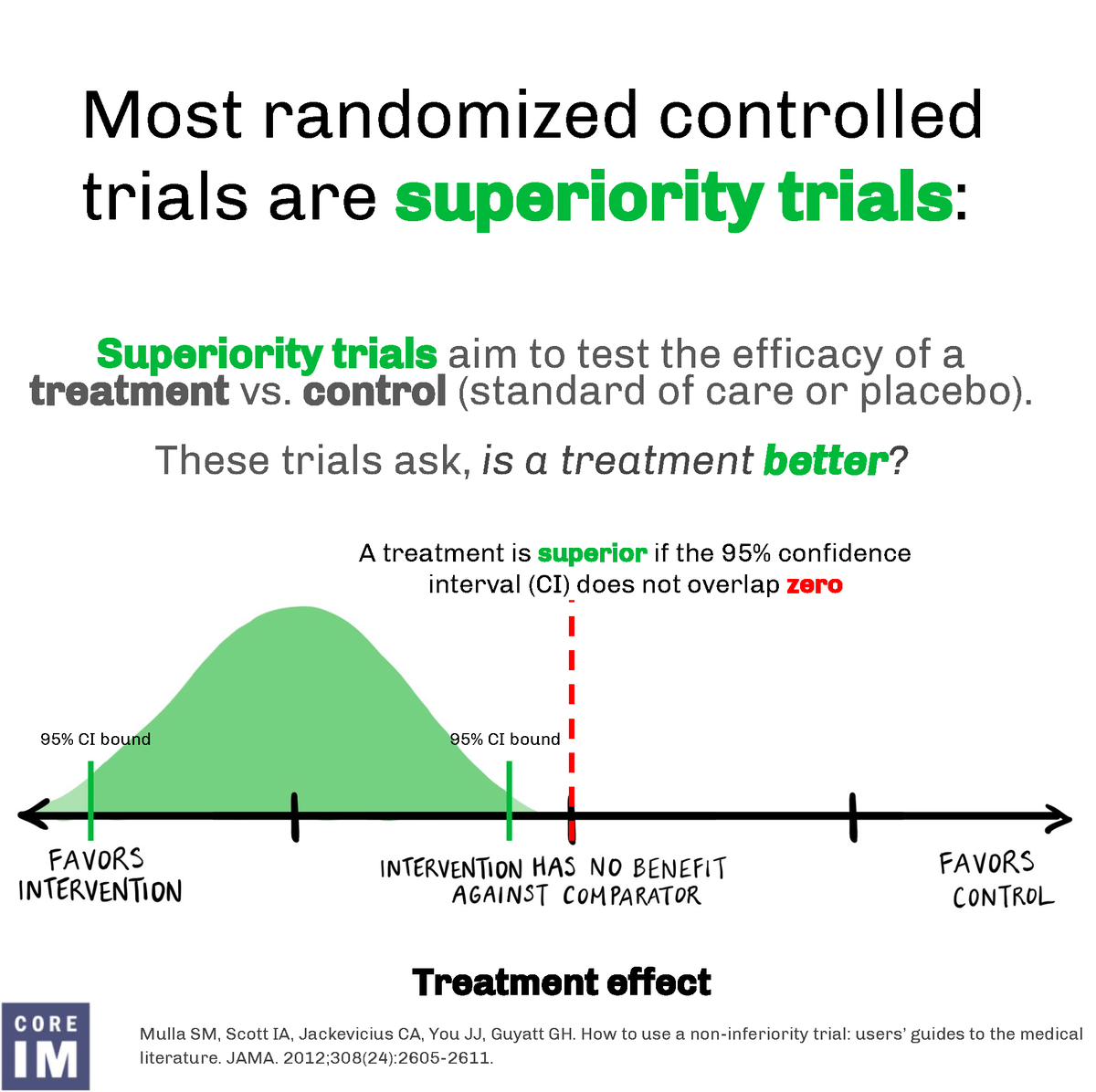
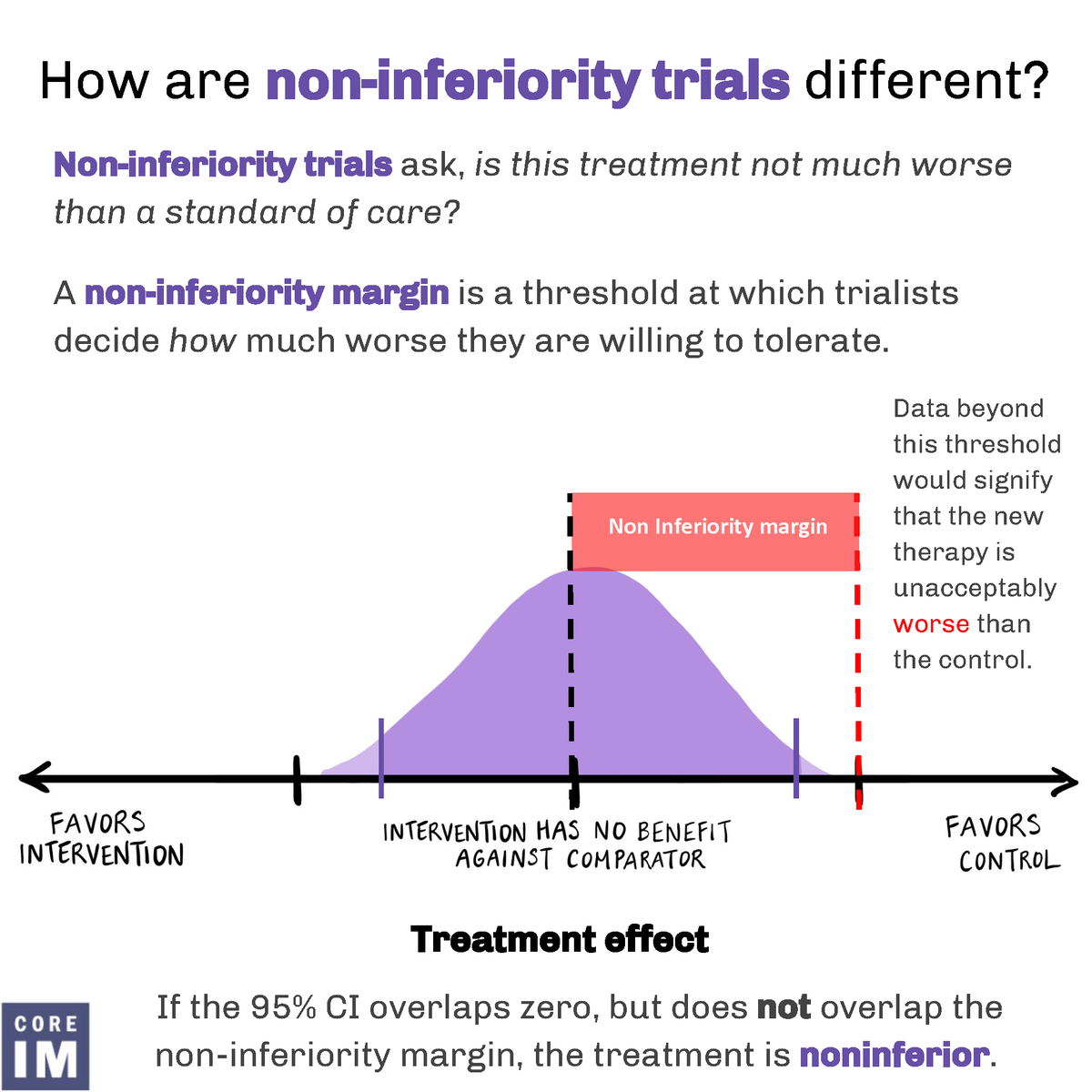
We can look to the STOPAH RCT for a decision to treat with steroids- But remember to r/o infection first!
We can look to the STOPAH RCT for a decision to treat with steroids- But remember to r/o infection first!

• • •
Missing some Tweet in this thread? You can try to
force a refresh