
1/ Want to continue the learning streak of #Kidneywk ?
#MedTwitter #NephTwitter, we bring another #ASPNFOAM group tweetorial based on pathology webinar @ASPNeph on T-cell mediated rejection(TCMR) in kidney transplant (Tx)
#MedTwitter #NephTwitter, we bring another #ASPNFOAM group tweetorial based on pathology webinar @ASPNeph on T-cell mediated rejection(TCMR) in kidney transplant (Tx)

2/
Let's start with a vignette! 13 yr M with CAKUT s/p DDKT 6mo ago, p/w with doubling of Cr from 0.7 to 1.5 mg/dl, normal vitals and PE. UA normal. A lot of recent stressors and concern for non-adherence.
Sounds like a familiar scenario?
Let's start with a vignette! 13 yr M with CAKUT s/p DDKT 6mo ago, p/w with doubling of Cr from 0.7 to 1.5 mg/dl, normal vitals and PE. UA normal. A lot of recent stressors and concern for non-adherence.
Sounds like a familiar scenario?
What is the potential cause of graft dysfunction in this patient?
3/ ⚡️Likely REJECTION!
Check out this awesome #tweetorial by @Miketurk6 on “SCARI” causes of kidney graft dysfunction🎃👻
Check out this awesome #tweetorial by @Miketurk6 on “SCARI” causes of kidney graft dysfunction🎃👻
https://twitter.com/michaelturk6/status/1433803586434125825?s=20&t=6bfPivLgznRMyD4NqomCYA
4/
📌Kidney transplant rejection remains an independent risk factor for long term graft survival.
📌Despite robust immunosuppression regimen, TCMR and antibody mediated rejection (ABMR) is a concerning cause for graft loss
pubmed.ncbi.nlm.nih.gov/32066593/
📌Kidney transplant rejection remains an independent risk factor for long term graft survival.
📌Despite robust immunosuppression regimen, TCMR and antibody mediated rejection (ABMR) is a concerning cause for graft loss
pubmed.ncbi.nlm.nih.gov/32066593/

5/
TCMR typically occurs in 1st yr post Tx.
ABMR is the most common cause of late kidney allograft failure.
pubmed.ncbi.nlm.nih.gov/34507254/
TCMR typically occurs in 1st yr post Tx.
ABMR is the most common cause of late kidney allograft failure.
pubmed.ncbi.nlm.nih.gov/34507254/
What are some risk factors for kidney Tx rejection?
6/
🧐Let’s look into histopathology of TCMR
😄This is a pathology webinar, duh!!!
Off we go to heavenly Banff🧳🏔️
🧐Let’s look into histopathology of TCMR
😄This is a pathology webinar, duh!!!
Off we go to heavenly Banff🧳🏔️

7/
🔤The Banff lingo
Banff Lesion Score
▶️Interstitial inflammation
-mononuclear infiltrates involving unscarred cortical parenchyma
▶️Tubulitis
-mononuclear infiltrates in tubular basement membrane
▶️Arteritis
- inflammatory cells beneath the endothelial cells
🔤The Banff lingo
Banff Lesion Score
▶️Interstitial inflammation
-mononuclear infiltrates involving unscarred cortical parenchyma
▶️Tubulitis
-mononuclear infiltrates in tubular basement membrane
▶️Arteritis
- inflammatory cells beneath the endothelial cells

8/
Banff classification
♦️Borderline rejection added 2005
♦️< 10-25% inflammation
♦️foci of tubulitis + minor interstitial inflammation (Banff i0 or i1)
♦️ interstitial inflammation (i2 or i3) with minor tubulitis (t1)
i0(t1-t3), i1(t1-t3), i2t1 and i2t3
tinyurl.com/yc29smb6
Banff classification
♦️Borderline rejection added 2005
♦️< 10-25% inflammation
♦️foci of tubulitis + minor interstitial inflammation (Banff i0 or i1)
♦️ interstitial inflammation (i2 or i3) with minor tubulitis (t1)
i0(t1-t3), i1(t1-t3), i2t1 and i2t3
tinyurl.com/yc29smb6

9/
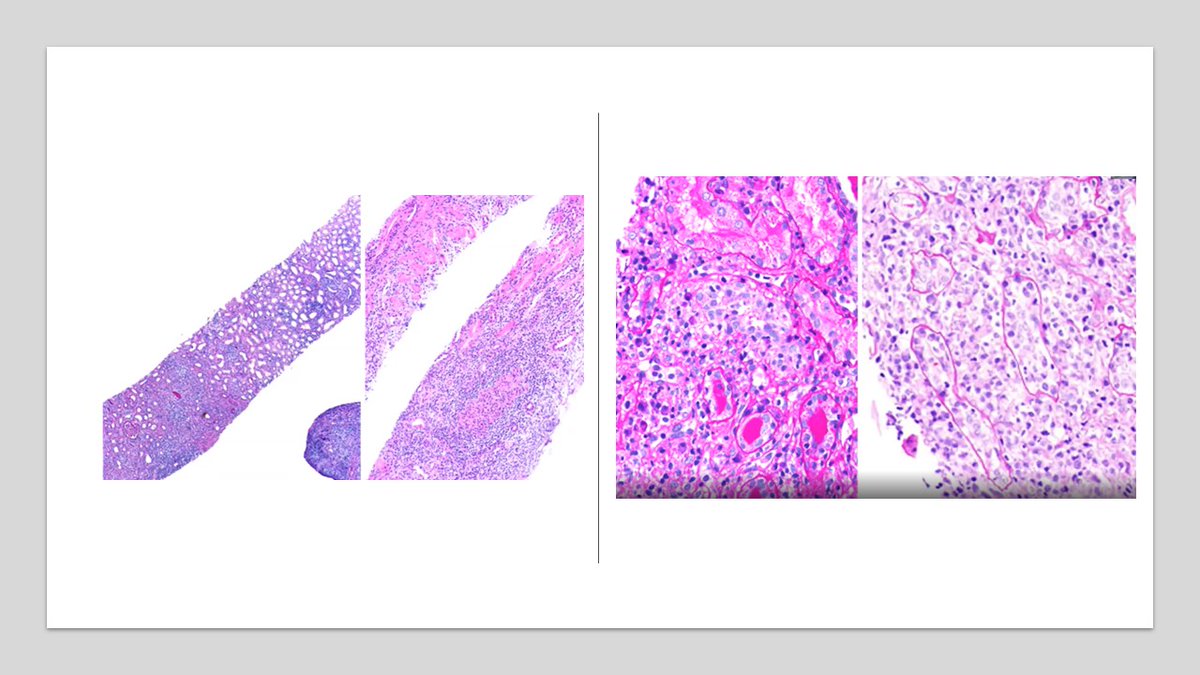
🔶Image shows mononuclear infiltrates in the interstitium, tubules and arteritis
🔶Light microscopy shows significant lymphocytic infiltrates
🔶Image shows mononuclear infiltrates in the interstitium, tubules and arteritis
🔶Light microscopy shows significant lymphocytic infiltrates

10/
💉Protocol biopsy done for early detection before change in GFR/proteinuria
🛑Pitfalls of biopsy(bx)
-Cost
-Invasive, potential complication
-Sampling error
-Labor intensive
renalfellow.org/2021/07/01/don… @RenalFellowNtwk @jadav_md
💉Protocol biopsy done for early detection before change in GFR/proteinuria
🛑Pitfalls of biopsy(bx)
-Cost
-Invasive, potential complication
-Sampling error
-Labor intensive
renalfellow.org/2021/07/01/don… @RenalFellowNtwk @jadav_md
What are the barriers to early diagnosis of kidney Tx rejection?
12/
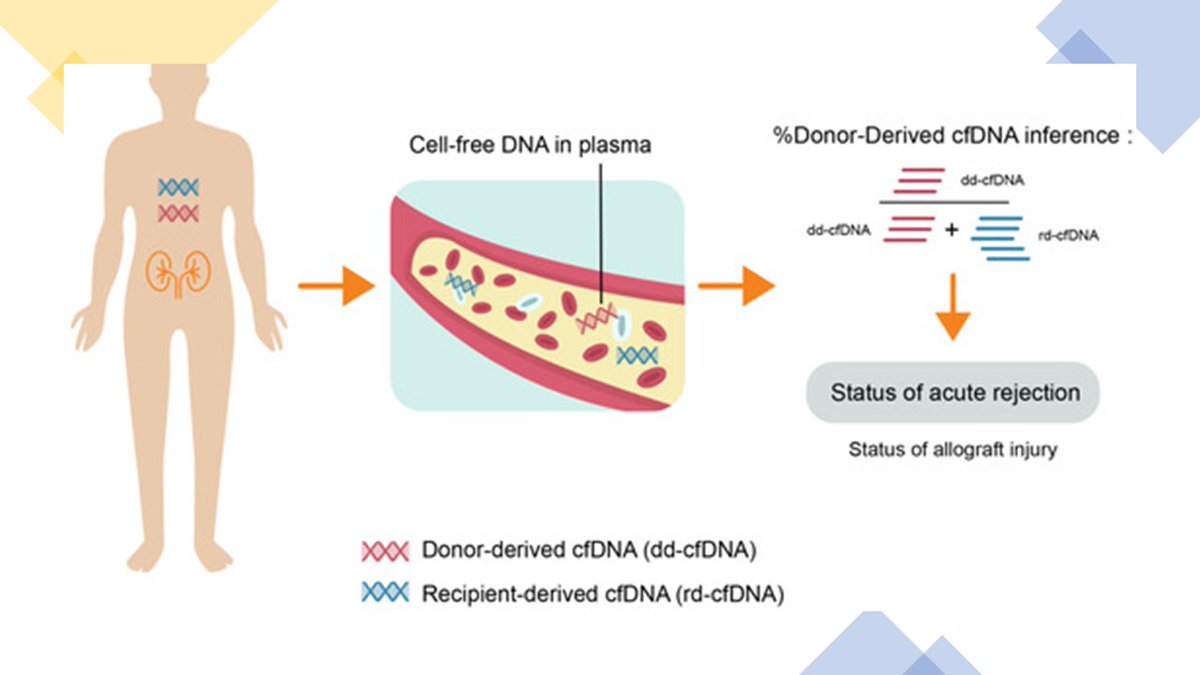
💥This calls for non-invasive bio-marker!!!
💠One such biomarker recently studied is donor derived cell free DNA
💠% or total amount DNA released from injured donor kidney tissue (DD cf-DNA)
mdpi.com/2077-0383/9/5/…
💥This calls for non-invasive bio-marker!!!
💠One such biomarker recently studied is donor derived cell free DNA
💠% or total amount DNA released from injured donor kidney tissue (DD cf-DNA)
mdpi.com/2077-0383/9/5/…
13/
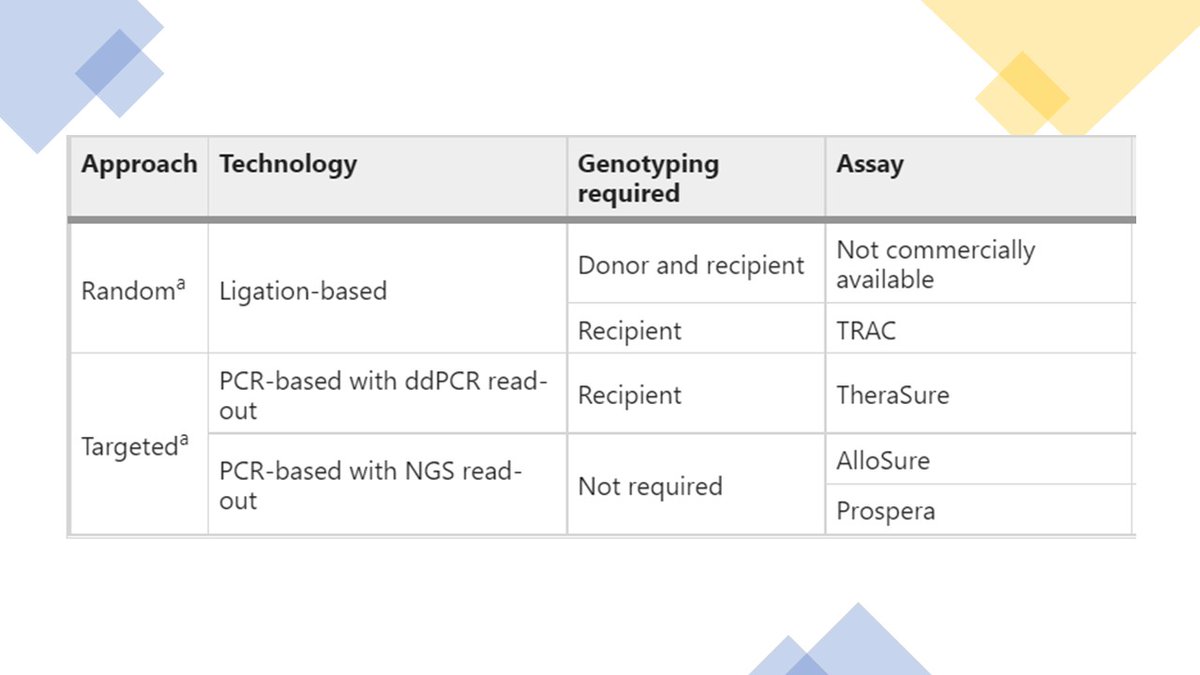
dd-cf-DNA clinical assay uses Single nucleotide polymorphism (SNP) for donor and recipient identification
Check out this article with beautiful cartoons @NatRevNeph
nature.com/articles/s4158…
dd-cf-DNA clinical assay uses Single nucleotide polymorphism (SNP) for donor and recipient identification
Check out this article with beautiful cartoons @NatRevNeph
nature.com/articles/s4158…
14/ Lets review few big studies on DD-cf-DNA
🎯DART-> Allosure testing platform
🔸Median dd-cfDNA in ABMR 2.9%;
🔸1.2% in TCMR grade 1B or worse
🔸0.2% for TCMR 1A
♦️ 1% cut-off used for test positivity
👉Better for predicting ABMR (AUC 0.87) than TCMR
PMID # 28280140
🎯DART-> Allosure testing platform
🔸Median dd-cfDNA in ABMR 2.9%;
🔸1.2% in TCMR grade 1B or worse
🔸0.2% for TCMR 1A
♦️ 1% cut-off used for test positivity
👉Better for predicting ABMR (AUC 0.87) than TCMR
PMID # 28280140
15/
♦️Initial Prospera study
🔸median cf-DNA for ABMR (2.2%), TCMR( 2.7%) and mixed rejection(2.6%) did not differ significantly.
pubmed.ncbi.nlm.nih.gov/30583588/
♦️Initial Prospera study
🔸median cf-DNA for ABMR (2.2%), TCMR( 2.7%) and mixed rejection(2.6%) did not differ significantly.
pubmed.ncbi.nlm.nih.gov/30583588/
16/
🧬Viracor Transplant Rejection Allograft Check(TRAC) analyzes 70,000 SNP’s, initial study promising with AUC for detection ~ 0.85
🧬Ongoing TRULO study looks at gene expression assay TruGraf and TRAC dd-cfDNA
tinyurl.com/52uva58f
🧬Viracor Transplant Rejection Allograft Check(TRAC) analyzes 70,000 SNP’s, initial study promising with AUC for detection ~ 0.85
🧬Ongoing TRULO study looks at gene expression assay TruGraf and TRAC dd-cfDNA
tinyurl.com/52uva58f
17/
Meta-analysis of cf-DNA in TCMR, the median level did not differ between pts with TCMR and those without rejection, thus limiting its utility
pubmed.ncbi.nlm.nih.gov/32981117/
Meta-analysis of cf-DNA in TCMR, the median level did not differ between pts with TCMR and those without rejection, thus limiting its utility
pubmed.ncbi.nlm.nih.gov/32981117/
18/
❓Why was cf-DNA not high in TCMR in these studies?
⚡️No direct endothelial injury
⚡️Mostly tubulointerstitial damage
⚡️Classifying TCMR into mixed rejection
❓Why was cf-DNA not high in TCMR in these studies?
⚡️No direct endothelial injury
⚡️Mostly tubulointerstitial damage
⚡️Classifying TCMR into mixed rejection
19/
▶️Borderline TCMR/1A rejection makes up ¾ of all ACR
▶️Does affect long term graft function
▶️cf-DNA could differentiate although at lower detection levels (<1%)
pubmed.ncbi.nlm.nih.gov/32056331/
▶️Borderline TCMR/1A rejection makes up ¾ of all ACR
▶️Does affect long term graft function
▶️cf-DNA could differentiate although at lower detection levels (<1%)
pubmed.ncbi.nlm.nih.gov/32056331/
20/
🔸Improvement in cf-DNA after IV pulse steroids for TCMR
💊Could be used to guide therapy
🧒Recent studies showed effectiveness of using cfDNA in ped kidney Tx
👇
PMID #
●36302566
●33217125
●35340104
🔸Improvement in cf-DNA after IV pulse steroids for TCMR
💊Could be used to guide therapy
🧒Recent studies showed effectiveness of using cfDNA in ped kidney Tx
👇
PMID #
●36302566
●33217125
●35340104
What the potential confounders of DD-cf-DNA?
21/
🔥Trifecta study in 300 kidney bx ->relationships b/w dd-cfDNA(%) at the time of indication biopsy and the genome-wide molecular findings assessed by microarrays
🔥Molecular rejection correlated with elevated cf-DNA better than histologic changes
tinyurl.com/4ef72pwm
🔥Trifecta study in 300 kidney bx ->relationships b/w dd-cfDNA(%) at the time of indication biopsy and the genome-wide molecular findings assessed by microarrays
🔥Molecular rejection correlated with elevated cf-DNA better than histologic changes
tinyurl.com/4ef72pwm
22/
Treatment TCMR
⚕️Banff BL, IA, IB→ Steroid pulse 10 mg/kg q daily x 3 doses OR oral steroid cycle over 3mo
⚕️Banff IIA,IIB, III→ Rabbit ATG 3-5 doses
Treatment TCMR
⚕️Banff BL, IA, IB→ Steroid pulse 10 mg/kg q daily x 3 doses OR oral steroid cycle over 3mo
⚕️Banff IIA,IIB, III→ Rabbit ATG 3-5 doses
23/
Chronic active TCMR is newly described entity with long term graft loss and variable treatment response
sciencedirect.com/science/articl…
Chronic active TCMR is newly described entity with long term graft loss and variable treatment response
sciencedirect.com/science/articl…

For a case-based clinical discussion on #TCMR with an expert - login to @ASPNeph website, Sept 2022 webinar #Membereducation
aspneph.org/committees/mem…
Special thanks to #ASPNFOAM group members @drM_sudha @CatherineJ20 for reviewing!
aspneph.org/committees/mem…
Special thanks to #ASPNFOAM group members @drM_sudha @CatherineJ20 for reviewing!

@threadreaderapp please unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh





