VIAGRA (Sildenafil) for #LongCovid or #MECFS?🧵
I've heard from several #pwLC & ME who reported their symptoms moderately to vastly improved following Viagra use.
Are these just wacky anecdotes or is there scientific basis for these positive effects?
Answer: the latter🧵
I've heard from several #pwLC & ME who reported their symptoms moderately to vastly improved following Viagra use.
Are these just wacky anecdotes or is there scientific basis for these positive effects?
Answer: the latter🧵
VIAGRA (sildenafil) & ME/CFS TRIAL
In 2008, Dr T Friedman hypothesized that Viagra would help ME/CFS patients by improving cerebral blood flow. He carried out a tiny placebo-controlled trial (n=12).
2/x
clinicaltrials.gov/ct2/show/NCT00…
In 2008, Dr T Friedman hypothesized that Viagra would help ME/CFS patients by improving cerebral blood flow. He carried out a tiny placebo-controlled trial (n=12).
2/x
clinicaltrials.gov/ct2/show/NCT00…
Change in Fatigue Impact Scale questionnaire suggested benefit with Viagra over placebo. However, only 5 on Viagra & 6 on placebo completed the trial & the study was never published.
Dosing:
Week 1: 25 mg TID*
Week 2: 50 mg TID
Weeks 3-6: 100 mg TID
*TID = 3 times daily
3/x
Dosing:
Week 1: 25 mg TID*
Week 2: 50 mg TID
Weeks 3-6: 100 mg TID
*TID = 3 times daily
3/x
Side note: Interestingly, sildenafil's mechanism of action shows similarities w vericiguat, a new oral heart failure drug currently being trialed in Long Covid patients (VERI-LONG trial). Both drugs ⬆️cGMP and promote smooth muscle relaxation & vasodilation.
4/x
4/x

The pathophysiology of heart failure (HF) shares similarities w/ Long Covid:
Endothelial dysfunction
Inflammation
Oxidative stress
Some HF symptoms are similar to LC & ME:
Fatigue & weakness
Exercise intolerance
Rapid or irregular heartbeat
Shortness of breath
et al
5/x
Endothelial dysfunction
Inflammation
Oxidative stress
Some HF symptoms are similar to LC & ME:
Fatigue & weakness
Exercise intolerance
Rapid or irregular heartbeat
Shortness of breath
et al
5/x
Read on for a quick overview of sildenafil's potential benefits in #LongCovid and/or #MECFS
1) Cognitive dysfunction
2a) Fatigue/exercise intolerance/hypoxia
2b) Shortness of breath/heart failure
3) Neuropathy
4) Endothelial dysfunction
5) Ischemic-perfusion injury(??)
6/x
1) Cognitive dysfunction
2a) Fatigue/exercise intolerance/hypoxia
2b) Shortness of breath/heart failure
3) Neuropathy
4) Endothelial dysfunction
5) Ischemic-perfusion injury(??)
6/x
1) COGNITIVE DYSFUNCTION
Sildenafil crosses the blood brain barrier & improves cerebral blood flow. Animal models found sildenafil to increase brain levels of cGMP which in turn promoted neurogenesis & reduced neurological deficits post acute stroke.
7/x
pubmed.ncbi.nlm.nih.gov/24034153/
Sildenafil crosses the blood brain barrier & improves cerebral blood flow. Animal models found sildenafil to increase brain levels of cGMP which in turn promoted neurogenesis & reduced neurological deficits post acute stroke.
7/x
pubmed.ncbi.nlm.nih.gov/24034153/
2a) FATIGUE/EXERCISE INTOLERANCE
Versus placebo, sildenafil (20, 40, or 80 mg) TID x 12 weeks improved exercise capacity, WHO functional class, quality of life, and hemodynamics in patients with symptomatic PAH.
8/x
nejm.org/doi/full/10.10…
Versus placebo, sildenafil (20, 40, or 80 mg) TID x 12 weeks improved exercise capacity, WHO functional class, quality of life, and hemodynamics in patients with symptomatic PAH.
8/x
nejm.org/doi/full/10.10…
2b) SHORTNESS OF BREATH/HEART FAILURE
Multiple small heart failure trials have shown sildenafil improved oxygen uptake, exercise capacity, cardiac output, breathlessness scores, & aerobic efficiency through 6 months.
(Recall preload failure recently found in MECFS @ Harvard)
9/x
Multiple small heart failure trials have shown sildenafil improved oxygen uptake, exercise capacity, cardiac output, breathlessness scores, & aerobic efficiency through 6 months.
(Recall preload failure recently found in MECFS @ Harvard)
9/x

3) NEUROPATHY
Daily use of sildenafil reduced neuropathic pain and paresthesias in several diabetes case studies. Hypothesis: sildenafil improved endothelial function & blood supply to vasa nervorum where peripheral nerves gain nourishment
10/x
pubmed.ncbi.nlm.nih.gov/16939556/
Daily use of sildenafil reduced neuropathic pain and paresthesias in several diabetes case studies. Hypothesis: sildenafil improved endothelial function & blood supply to vasa nervorum where peripheral nerves gain nourishment
10/x
pubmed.ncbi.nlm.nih.gov/16939556/

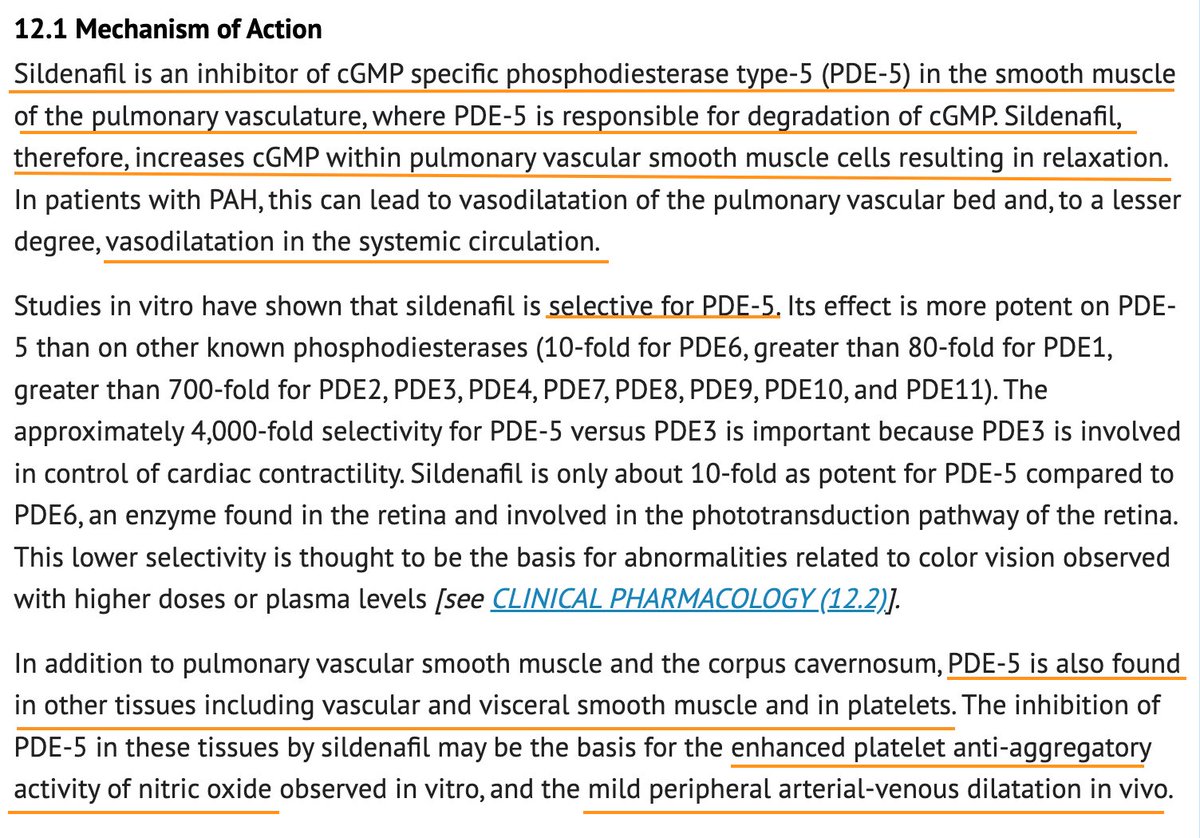
4) ENDOTHELIAL DYSFUNCTION
RCT in prediabetic adults: Sildenafil significantly improved insulin sensitivity index, ⬇️ PAI-1 & ⬇️ACR (albumin/creatinine ratio), suggesting better fibrinolytic balance and improved endothelial function.
11/x
ncbi.nlm.nih.gov/pmc/articles/P…
RCT in prediabetic adults: Sildenafil significantly improved insulin sensitivity index, ⬇️ PAI-1 & ⬇️ACR (albumin/creatinine ratio), suggesting better fibrinolytic balance and improved endothelial function.
11/x
ncbi.nlm.nih.gov/pmc/articles/P…
5) ISCHEMIC-PERFUSION INJURY??
Not so confident on this one (limited to animal studies) but worth mentioning: Multiple animal studies have found that sildenafil induces acute & delayed protective effects against ischemia-reperfusion injury.
12/x
pubmed.ncbi.nlm.nih.gov/26850186/
Not so confident on this one (limited to animal studies) but worth mentioning: Multiple animal studies have found that sildenafil induces acute & delayed protective effects against ischemia-reperfusion injury.
12/x
pubmed.ncbi.nlm.nih.gov/26850186/
Turns out I am not the only one thinking of PDE5 inhibitors for Long Covid: This MD wrote an editorial advocating for sildenafil in #LongCovid patients with dyspnea (difficult breathing).
13/x
journals.lww.com/americantherap…
13/x
journals.lww.com/americantherap…
Am I saying to go out & get an Rx for Viagra stat?
No!
But I DO think this is an avenue worth further study.
Some already take these meds for other uses. So, a poll:
Since Long Covid or ME/CFS, has use of PDE5 inhibitors (Viagra, Cialis, Revatio) helped your LC or ME?
end🧵
No!
But I DO think this is an avenue worth further study.
Some already take these meds for other uses. So, a poll:
Since Long Covid or ME/CFS, has use of PDE5 inhibitors (Viagra, Cialis, Revatio) helped your LC or ME?
end🧵
Some closing notes:
1 of 2:
Sildenafil is typically effective within 30-60 minutes of administration. Half-life = 4 hrs & duration of action up to 12 hrs. Fatty meals will reduce absorption & thus efficacy.
1 of 2:
Sildenafil is typically effective within 30-60 minutes of administration. Half-life = 4 hrs & duration of action up to 12 hrs. Fatty meals will reduce absorption & thus efficacy.
2) Relevant side effects/cautions
PDE5Is like Viagra may lower BP.
Dysautonomia exacerbation possible‼️ (unknown how lilkely)
Avoid with other nitrates or strong CYP3A4 inhibitors (including Paxlovid).
Visual disturbances: avoid if h/o NAION, melanoma
Hearing loss or tinnitus ⁉️
PDE5Is like Viagra may lower BP.
Dysautonomia exacerbation possible‼️ (unknown how lilkely)
Avoid with other nitrates or strong CYP3A4 inhibitors (including Paxlovid).
Visual disturbances: avoid if h/o NAION, melanoma
Hearing loss or tinnitus ⁉️


Postscript on tadalafil (Cialis), another PDE5I:
15 yrs ago, a poster presentation showed that tadalafil 20 mg every 3 days for 5 doses improved shortness of breath & fatigue after exercise in 27 of 30 #MECFS male patients. Authors believed PDE5I efficacy may be related to PAP.
15 yrs ago, a poster presentation showed that tadalafil 20 mg every 3 days for 5 doses improved shortness of breath & fatigue after exercise in 27 of 30 #MECFS male patients. Authors believed PDE5I efficacy may be related to PAP.

• • •
Missing some Tweet in this thread? You can try to
force a refresh