#MedTwitter #HemeBoards @HemOncFellows
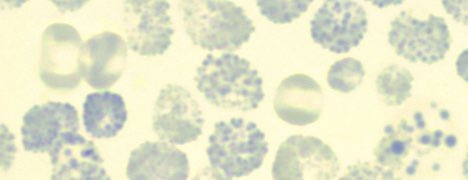
🧵Summary of erythrocytes inclusion bodies:
1️⃣Howell-Jolly body
➡️composition: DNA
🔬associations: splenectomy, hyposplenism, megaloblastic anemia, hemolytic anemia, sickle cell disease
🧵Summary of erythrocytes inclusion bodies:
1️⃣Howell-Jolly body
➡️composition: DNA
🔬associations: splenectomy, hyposplenism, megaloblastic anemia, hemolytic anemia, sickle cell disease

2️⃣Basophilic stippling
➡️composition: RNA
🔬associations: lead intoxication, thalassemia, abnormal heme synthesis
➡️composition: RNA
🔬associations: lead intoxication, thalassemia, abnormal heme synthesis

3️⃣Pappenheimer bodies
➡️composition: iron
🔬associations: splenectomy, hemolytic anemia, sideroblastic anemia, megaloblastic anemia, hemoglobinopathies
➡️composition: iron
🔬associations: splenectomy, hemolytic anemia, sideroblastic anemia, megaloblastic anemia, hemoglobinopathies

4️⃣Cabbot ring
➡️composition: remanent of mitosis spindle
🔬associations: MDS, megaloblastic anemia, AML
➡️composition: remanent of mitosis spindle
🔬associations: MDS, megaloblastic anemia, AML

5️⃣Heinz body
➡️composition: unstable haemoglobin
🔬associations: unstable hemoglobin, G6PD deficiency and other erythrocytes enzyme deficiency, some hemoglobinopathies, alpha thalassemia
➡️composition: unstable haemoglobin
🔬associations: unstable hemoglobin, G6PD deficiency and other erythrocytes enzyme deficiency, some hemoglobinopathies, alpha thalassemia

6️⃣Hemoglobin H
➡️composition: beta chain tetramers
🔬associations: a type of alpha thalassemia
End🧵
➡️composition: beta chain tetramers
🔬associations: a type of alpha thalassemia
End🧵
• • •
Missing some Tweet in this thread? You can try to
force a refresh