Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣ classic Hodgkin's lymphoma
🩸Reed-Sternberg cell👇
🩸Most common: Nodular sclerosis 👇(fibrosis)
🩸Usually:CD30+, CD15+, weak PAX5 +. CD20-, CD45-
🩸9p24.1 alteration
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣ classic Hodgkin's lymphoma
🩸Reed-Sternberg cell👇
🩸Most common: Nodular sclerosis 👇(fibrosis)
🩸Usually:CD30+, CD15+, weak PAX5 +. CD20-, CD45-
🩸9p24.1 alteration


Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
2⃣ Nodular lymphocyte-predominant Hodgkin lymphoma
🩸popcorn cell (from germinal center B-cell)👇
🩸CD20+ (different than cHL),Rituxan used in ttt
🩸can transform(DLBCL)
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
2⃣ Nodular lymphocyte-predominant Hodgkin lymphoma
🩸popcorn cell (from germinal center B-cell)👇
🩸CD20+ (different than cHL),Rituxan used in ttt
🩸can transform(DLBCL)

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
3⃣ Follicular lymphoma
🩸Bone marrow with small lymphocytes👇
🩸CD20+,CD10+,BCL6+,BCL2+,CD5-
🩸t(14;18) in up to 90% of cases
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
3⃣ Follicular lymphoma
🩸Bone marrow with small lymphocytes👇
🩸CD20+,CD10+,BCL6+,BCL2+,CD5-
🩸t(14;18) in up to 90% of cases

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
4⃣ Splenic marginal zone lymphoma
🩸Spindle cell👇
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
4⃣ Splenic marginal zone lymphoma
🩸Spindle cell👇

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
5⃣ Burkitt lymphoma
🩸Starry sky appearance👇(can occur in other high grade B-cell lymphoma)
🩸vacuolated cells with deep basophilic cytoplasm👇
🩸t(8;14)(q24;q32):MYC
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
5⃣ Burkitt lymphoma
🩸Starry sky appearance👇(can occur in other high grade B-cell lymphoma)
🩸vacuolated cells with deep basophilic cytoplasm👇
🩸t(8;14)(q24;q32):MYC


Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
6⃣ MDS
🩸Dysplastic megakaryocytes (widely separated nuclear lobes)👇
🩸Ring sideroblasts, typically SF3B1 mutation👇
🩸Dysplastic neutrophil (hypolobation,hypogranular)👇
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
6⃣ MDS
🩸Dysplastic megakaryocytes (widely separated nuclear lobes)👇
🩸Ring sideroblasts, typically SF3B1 mutation👇
🩸Dysplastic neutrophil (hypolobation,hypogranular)👇



Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
7⃣ MM-1
🩸plasma cells in BM👇
🩸Rouleaux&circulating plasma cells👇
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
7⃣ MM-1
🩸plasma cells in BM👇
🩸Rouleaux&circulating plasma cells👇


Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
7⃣ MM-2
🩸Russell bodies(intracytoplasmic)/ Mott/Grape cell👇
🩸Dutcher body(intranuclear)👇: can occur in LPL/Waldenstorm's, MYD88+
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
7⃣ MM-2
🩸Russell bodies(intracytoplasmic)/ Mott/Grape cell👇
🩸Dutcher body(intranuclear)👇: can occur in LPL/Waldenstorm's, MYD88+


Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
8⃣ Essential thrombocythemia
🩸mutations: JAK2,CALR,MPL
🩸Smear with thrombocytosis👇
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
8⃣ Essential thrombocythemia
🩸mutations: JAK2,CALR,MPL
🩸Smear with thrombocytosis👇

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
8⃣ Primary myelofibrosis
🩸Tear drop cells (dacrocytes) 👇 with a blast in the center
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
8⃣ Primary myelofibrosis
🩸Tear drop cells (dacrocytes) 👇 with a blast in the center

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
9⃣ Eosinophils in the setting of FIPL1-PDFGRA rearrangement
🩸Hypereosinophilia
🩸CHIC2 gene (FISH or PCR)- cytogenetics does not pick it
🩸Responds well to imatinib
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
9⃣ Eosinophils in the setting of FIPL1-PDFGRA rearrangement
🩸Hypereosinophilia
🩸CHIC2 gene (FISH or PCR)- cytogenetics does not pick it
🩸Responds well to imatinib

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
🔟Systemic mastocytosis
🩸Spindly mast cell clusters👇
🩸KIT D816V mutation is most common
⭐️Elevated tryptase levels
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
🔟Systemic mastocytosis
🩸Spindly mast cell clusters👇
🩸KIT D816V mutation is most common
⭐️Elevated tryptase levels

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣1⃣Hairy cell leukemia
🩸hairy cells👇
🩸CD11c+,CD22+,CD25+.CD103+
🩸BRAF V600E mutation
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣1⃣Hairy cell leukemia
🩸hairy cells👇
🩸CD11c+,CD22+,CD25+.CD103+
🩸BRAF V600E mutation
Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣2⃣ CLL
🩸small lymphocytes/soccer ball/cobblestone pattern👇
🩸Smudge/basket cells: cells fragile and get smudged when smear is prepared👇
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣2⃣ CLL
🩸small lymphocytes/soccer ball/cobblestone pattern👇
🩸Smudge/basket cells: cells fragile and get smudged when smear is prepared👇


Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣3⃣CMML
🩸MDS/MPN overlap syndrome
🩸monocytes (needs absolute monocytosis >1000 monocyte per mL)
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣3⃣CMML
🩸MDS/MPN overlap syndrome
🩸monocytes (needs absolute monocytosis >1000 monocyte per mL)

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣4⃣Adult T cell leukemia/lymphoma(ATIL)
🩸associated with hypercalcemia and spastic paraparesis
🩸HTLV-1 infection, endemic in the Carribean and Japan
🩸Flower cells 👇
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣4⃣Adult T cell leukemia/lymphoma(ATIL)
🩸associated with hypercalcemia and spastic paraparesis
🩸HTLV-1 infection, endemic in the Carribean and Japan
🩸Flower cells 👇

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
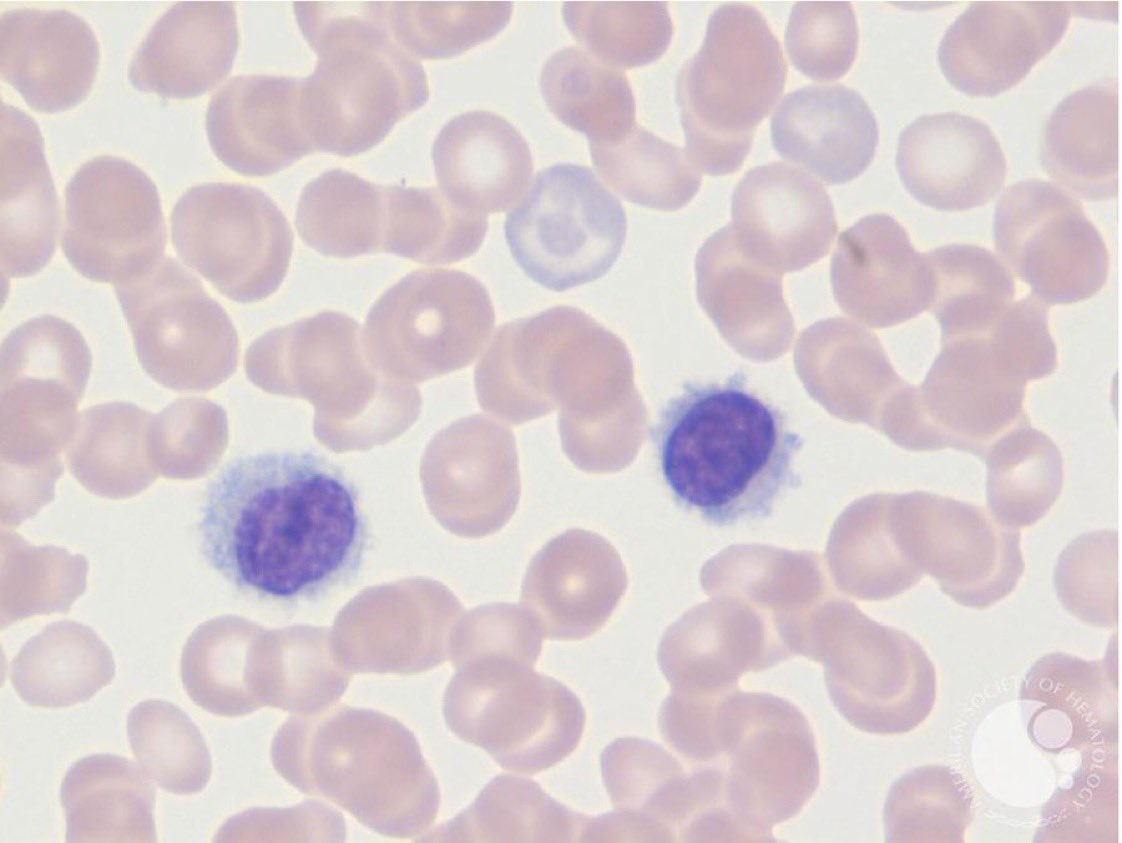
1⃣5⃣ Sezary syndrome
🩸Mature T-cell Leukemia
🩸Sezary cell 👇 CD3+/CD4+
🩸erythroderma, generalized lymphadenopathy
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣5⃣ Sezary syndrome
🩸Mature T-cell Leukemia
🩸Sezary cell 👇 CD3+/CD4+
🩸erythroderma, generalized lymphadenopathy

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
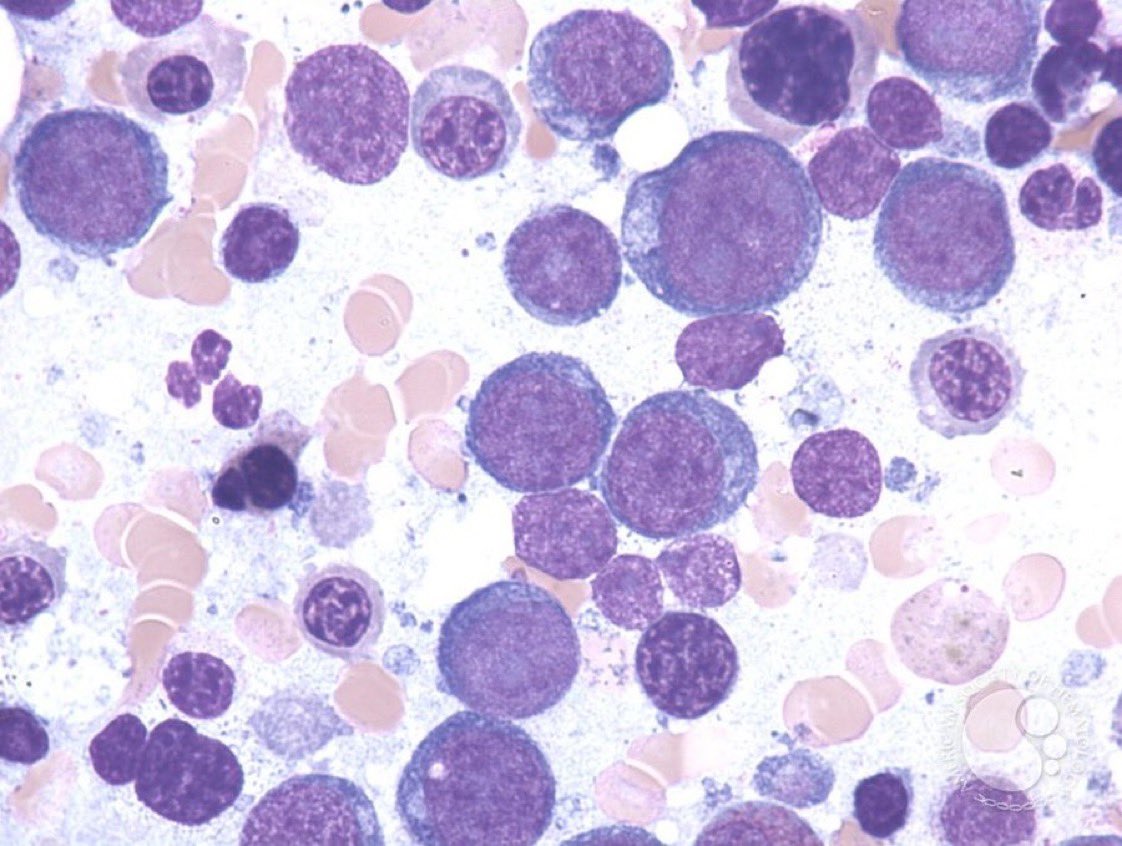
1⃣6⃣Acute erythroid leukemia
🩸glycophorin A-positive neoplastic cells in BM (Glycophorins=erythroid)
🩸Proerythroblasts: large cells with immature basophilic cytoplasm👇
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣6⃣Acute erythroid leukemia
🩸glycophorin A-positive neoplastic cells in BM (Glycophorins=erythroid)
🩸Proerythroblasts: large cells with immature basophilic cytoplasm👇
Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣7⃣ B-ALL
🩸CD10+,CD19+ (B-cell lineage), CD34+ (immature blastic phenotype)
🩸Myeloid associated markers: CD13+,CD33+,MPO-
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣7⃣ B-ALL
🩸CD10+,CD19+ (B-cell lineage), CD34+ (immature blastic phenotype)
🩸Myeloid associated markers: CD13+,CD33+,MPO-

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣8⃣ Acute megakaryoblastic leukemia
🩸Megakaryoblasts👇Large,cytoplasmic blebbing,pseudopod formation-granular basophilic cytoplasm
🩸CD41+(glycoprotein IIb/IIIa)&CD61+
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣8⃣ Acute megakaryoblastic leukemia
🩸Megakaryoblasts👇Large,cytoplasmic blebbing,pseudopod formation-granular basophilic cytoplasm
🩸CD41+(glycoprotein IIb/IIIa)&CD61+

Blood smears @ASH_hematology 🧵Heme boards
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣9⃣ Acute promyelocytic leukemia
🩸Auer rods👇
🩸Faggot cell (many auer rods together)👇
🩸t(15;17), PML-RARA
🩸Malignant Hematopoietic Neoplasms🩸
#mmsm #lymsm #leusm #bmtsm
1⃣9⃣ Acute promyelocytic leukemia
🩸Auer rods👇
🩸Faggot cell (many auer rods together)👇
🩸t(15;17), PML-RARA


End 🧵
Peripheral blood smear is important both for boards and for real life:
hematology.org/education/trai…
Peripheral blood smear is important both for boards and for real life:
hematology.org/education/trai…
• • •
Missing some Tweet in this thread? You can try to
force a refresh