
I get asked all the time: Can MRD status guide treatment decision in myeloma?
📜A separate thread dedicated to #ASH22 studies investigating #mmMRD-guided management in myeloma.
I will post lots more about our MRD2STOP study as we get closer to the conference! #mmsm
📜A separate thread dedicated to #ASH22 studies investigating #mmMRD-guided management in myeloma.
I will post lots more about our MRD2STOP study as we get closer to the conference! #mmsm
Abstract 992 (@kordeneha1):
The premise: Patients with 3+ years of MRD-neg (flow, 10^-5 to 10^-6) undergo discontinuation of maintenance. Monitored q6mos bone marrow (flow), yearly PET.
n=23
👍Sustained MRD-neg at 12 months: 14/16 (88%)
👍12 month PFS: 94%
ashpublications.org/blood/article/…
The premise: Patients with 3+ years of MRD-neg (flow, 10^-5 to 10^-6) undergo discontinuation of maintenance. Monitored q6mos bone marrow (flow), yearly PET.
n=23
👍Sustained MRD-neg at 12 months: 14/16 (88%)
👍12 month PFS: 94%
ashpublications.org/blood/article/…

Abstract 3237 (@End_myeloma) Update from MASTER trial (MRD-Adapted Dara-KRd + ASCT):
#⃣84 pts in treatment-free surveillance, f/u ~24 mos.
👉8% MRD resurgence, 13% disease progression
☀️79% still off treatment
⚠️Only 47% of ultra-high risk pts off therapy
ash.confex.com/ash/2022/webpr…
#⃣84 pts in treatment-free surveillance, f/u ~24 mos.
👉8% MRD resurgence, 13% disease progression
☀️79% still off treatment
⚠️Only 47% of ultra-high risk pts off therapy
ash.confex.com/ash/2022/webpr…

Abstract 3247 (@KarenSweiss)
Screening pts to confirm sustained MRD-neg before stopping maintenance. Follow yearly w/MRD & tumor microenvironment in marrow, mass spec & circulating plasma cells in blood.
n=11 pts screened, 7 MRD-negative at baseline. ash.confex.com/ash/2022/webpr…
Screening pts to confirm sustained MRD-neg before stopping maintenance. Follow yearly w/MRD & tumor microenvironment in marrow, mass spec & circulating plasma cells in blood.
n=11 pts screened, 7 MRD-negative at baseline. ash.confex.com/ash/2022/webpr…
Abstract 4564 (Ailawadhi)
Daratumumab x 2-4 cycles if MRD(+) after induction (b4 ASCT). Dara-Len as maintenance.
👉15% converted to MRD-neg w/dara.
👍ASCT major impact on conversion to MRD-neg
⚠️Sustained MRD-neg looks low but many results pending doi.org/10.1182/blood-…
Daratumumab x 2-4 cycles if MRD(+) after induction (b4 ASCT). Dara-Len as maintenance.
👉15% converted to MRD-neg w/dara.
👍ASCT major impact on conversion to MRD-neg
⚠️Sustained MRD-neg looks low but many results pending doi.org/10.1182/blood-…

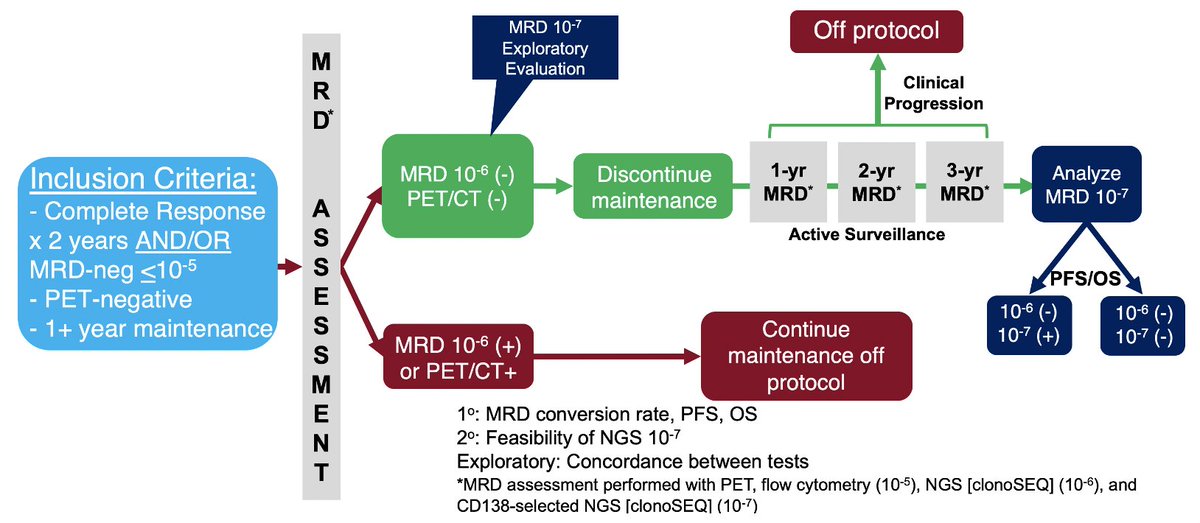
Abstract 870 (MRD2STOP)
Stop treatment in pts w/undetectable disease by clonoSEQ (10^-6), flow (10^-5), PET/CT, & 1+ years of maint.
Exploratory: 10^-7 assay (marrow), mass spec & cfDNA (blood)
Sustained MRD-neg @ 12 mos:
10^-6: 21/25 (84%)
10^-7: 20/21 (95%)
Tune in Monday!
Stop treatment in pts w/undetectable disease by clonoSEQ (10^-6), flow (10^-5), PET/CT, & 1+ years of maint.
Exploratory: 10^-7 assay (marrow), mass spec & cfDNA (blood)
Sustained MRD-neg @ 12 mos:
10^-6: 21/25 (84%)
10^-7: 20/21 (95%)
Tune in Monday!
• • •
Missing some Tweet in this thread? You can try to
force a refresh



