Today 1990 saw the @NobelPrize lecture by Donnall Thomas @fredhutch: "Bone Marrow Transplantation - Past, Present and Future"
Time to reflect upon a story of contradiction, disappointment, hope & love for medicine, science & improving patients' lives.
A short🧵
#Medtwitter
Time to reflect upon a story of contradiction, disappointment, hope & love for medicine, science & improving patients' lives.
A short🧵
#Medtwitter

1/
Darkness:
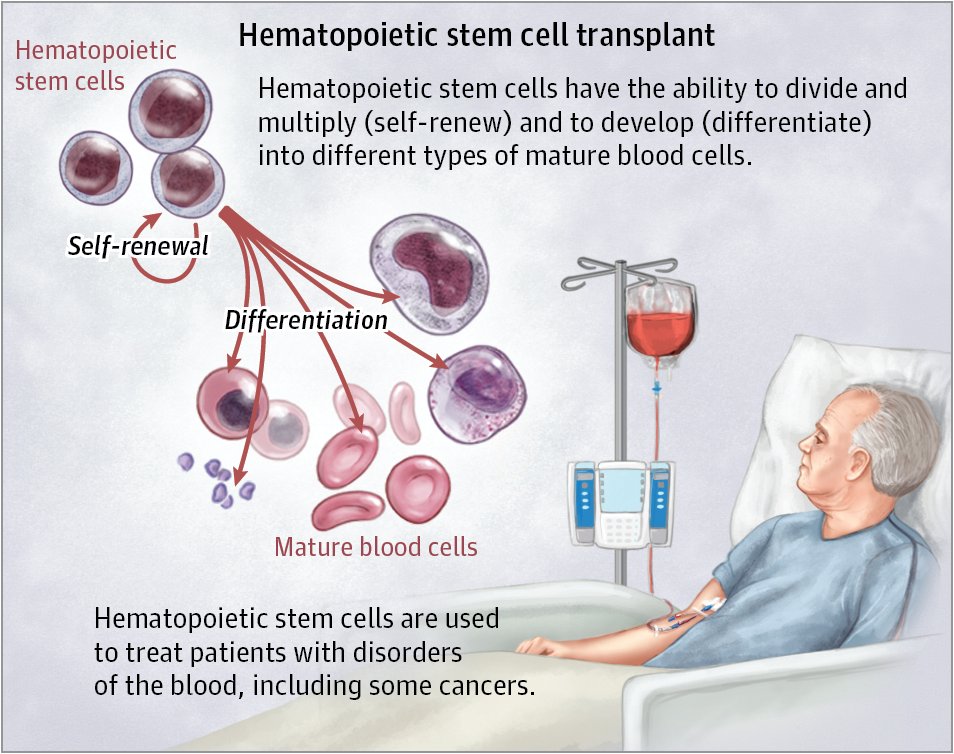
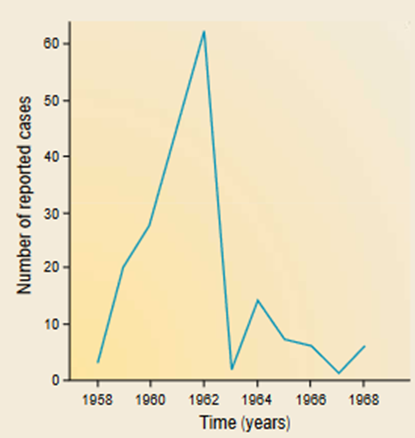
In late ‘40s, major research efforts were directed at repairing radiation damage to organs in response to observations in survivors of the horrific atomic bomb explosions in Japan. Leukaemia was the 1st cancer associated with atomic bomb radiation exposure.
Darkness:
In late ‘40s, major research efforts were directed at repairing radiation damage to organs in response to observations in survivors of the horrific atomic bomb explosions in Japan. Leukaemia was the 1st cancer associated with atomic bomb radiation exposure.

2/
Results of a study in '49 showed protection of mice given an otherwise lethal dose by shielding of the spleen during the irradiation. This procedure caused an impressive reduction in mortality, and moreover the spleen appeared to be specific in this respect.
Reviewed in 👇
Results of a study in '49 showed protection of mice given an otherwise lethal dose by shielding of the spleen during the irradiation. This procedure caused an impressive reduction in mortality, and moreover the spleen appeared to be specific in this respect.
Reviewed in 👇

3/
Humoral?
Many researchers believed that radiation protection was due to some humoral factor present in spleen or bone marrow, a controversial supposition and not shared by others who thought the ‘rescue’ of the irradiated mice had cellular origins.
Humoral?
Many researchers believed that radiation protection was due to some humoral factor present in spleen or bone marrow, a controversial supposition and not shared by others who thought the ‘rescue’ of the irradiated mice had cellular origins.
4/
No, cellular!
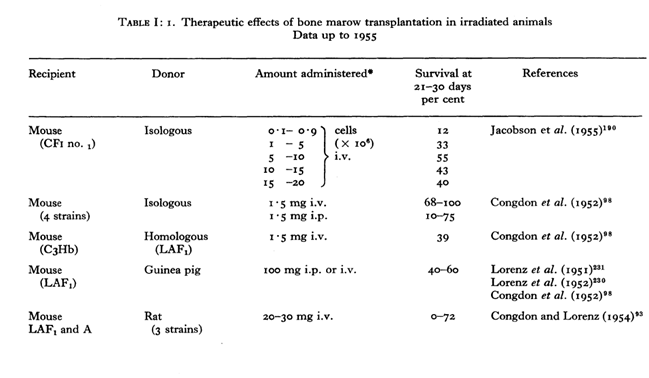
Until the mid-1950s several laboratories unequivocally documented, with the help of blood genetic markers, that radioprotection was due to repopulation of irradiated marrow spaces by transplanted donor cells.
No, cellular!
Until the mid-1950s several laboratories unequivocally documented, with the help of blood genetic markers, that radioprotection was due to repopulation of irradiated marrow spaces by transplanted donor cells.
The big hit:
In 1957, Donnall Thomas et al. reported @NEJM that marrow could be infused into irradiated leukemia patients and then engraft, even though, in the end, the patients were not cured of their leukemia.
In 1957, Donnall Thomas et al. reported @NEJM that marrow could be infused into irradiated leukemia patients and then engraft, even though, in the end, the patients were not cured of their leukemia.

6/
Something we hate and admire:
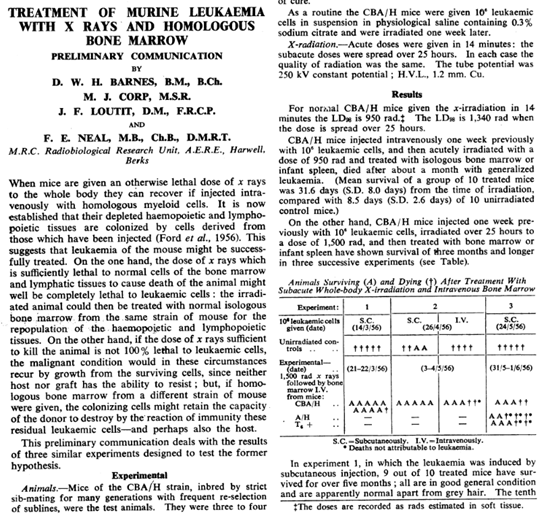
Previously, in 1956 Barnes et al. also showed in mice that an effect called "secondary disease" after marrow infusion could lead to eradication of leukemic cells. Effects now called "graft-versus-host” & “graft-versus-leukemia were born.
Something we hate and admire:
Previously, in 1956 Barnes et al. also showed in mice that an effect called "secondary disease" after marrow infusion could lead to eradication of leukemic cells. Effects now called "graft-versus-host” & “graft-versus-leukemia were born.
7/
A hard lesson:
Excitement led to more studies but many errors in extrapolation from the laboratory experiment to the patient have been made and much time was lost before it became evident that GVHD in primates is more violent than in rodents. Disappointment grew...
A hard lesson:
Excitement led to more studies but many errors in extrapolation from the laboratory experiment to the patient have been made and much time was lost before it became evident that GVHD in primates is more violent than in rodents. Disappointment grew...
8/
In ’64, Mathé et al. described a leukemia case after TBI + marrow infusion from 6 relatives. The marrow of 1 relative engrafted. While the patient eventually succumbed to GVHD his leukemia remained in remission (GVL). Modern-day "adoptive immunotherapy" was coined.
In ’64, Mathé et al. described a leukemia case after TBI + marrow infusion from 6 relatives. The marrow of 1 relative engrafted. While the patient eventually succumbed to GVHD his leukemia remained in remission (GVL). Modern-day "adoptive immunotherapy" was coined.
9/
The ones that stayed on the ship:
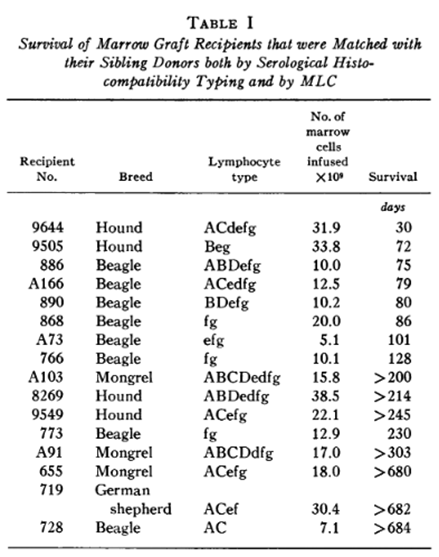
Many left the field. But an unexpected observation by Storb et al. in a canine experiment was that GVHD developed in minor histocompatibility class (MHC) matched littermates, even though significantly later than in mismatched littermates.
The ones that stayed on the ship:
Many left the field. But an unexpected observation by Storb et al. in a canine experiment was that GVHD developed in minor histocompatibility class (MHC) matched littermates, even though significantly later than in mismatched littermates.
10/
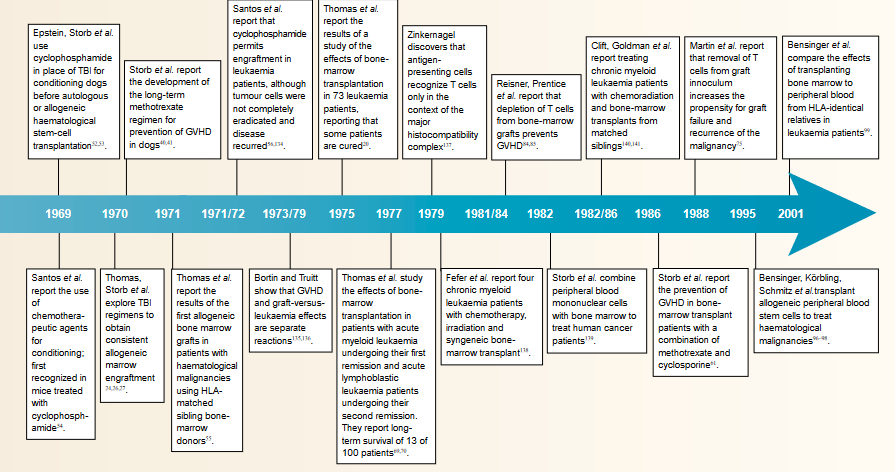
Let’s recap our 25 year sprint through the beginnings of BMT.
Let’s recap our 25 year sprint through the beginnings of BMT.

11/
GVHD is the enemy:
How to prevent GVHD in well-matched donor-recipient BMT?
👉studies of numerous immunosuppressive agents were conducted in ‘70s in a canine model that eventually led to identifying the antimetabolite methotrexate as the best drug for GVHD prevention.
GVHD is the enemy:
How to prevent GVHD in well-matched donor-recipient BMT?
👉studies of numerous immunosuppressive agents were conducted in ‘70s in a canine model that eventually led to identifying the antimetabolite methotrexate as the best drug for GVHD prevention.

12/
Riding on the storm:
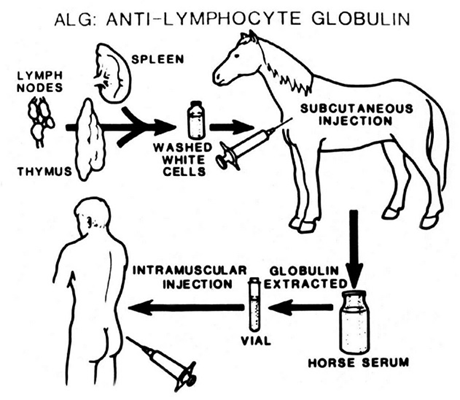
A more immunosuppressive regimen was developed that combined antithymocyte globulin (ATG, from horse or rabbit) with cyclophosphamide.
This regimen has then become standard practice for aplastic anemia patients with HLA-identical sibling donors.
Riding on the storm:
A more immunosuppressive regimen was developed that combined antithymocyte globulin (ATG, from horse or rabbit) with cyclophosphamide.
This regimen has then become standard practice for aplastic anemia patients with HLA-identical sibling donors.
13/
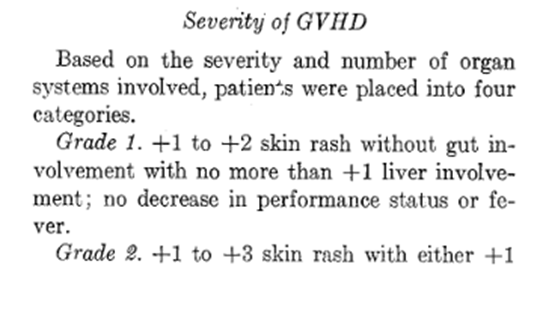
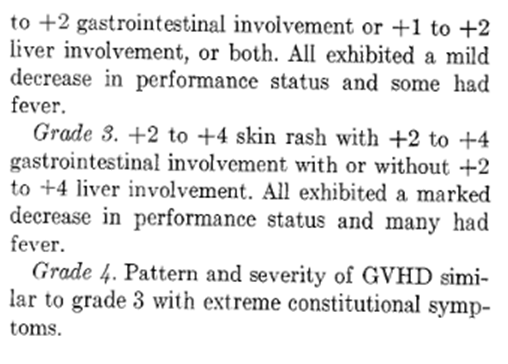
Grading the ungrateful:
In 1974, the 1st grading system for acute GVHD was described and its 1st effective treatment ATG was reported ATG was not commercially available and thus produced in single laboratories by immunizing rabbits with human thymocytes.
Grading the ungrateful:
In 1974, the 1st grading system for acute GVHD was described and its 1st effective treatment ATG was reported ATG was not commercially available and thus produced in single laboratories by immunizing rabbits with human thymocytes.
14/
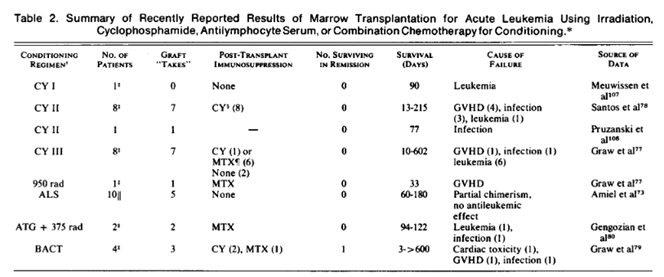
Return of the shadow:
Many patients still died from relapse but transplanting earlier in disease course reduced the relapse risk and led to a significant improvement in survival among patients with acute leukemia.
Return of the shadow:
Many patients still died from relapse but transplanting earlier in disease course reduced the relapse risk and led to a significant improvement in survival among patients with acute leukemia.
15/
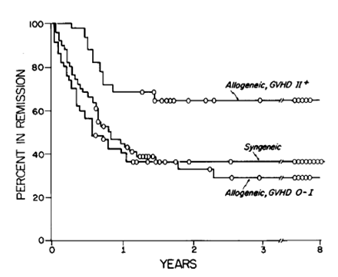
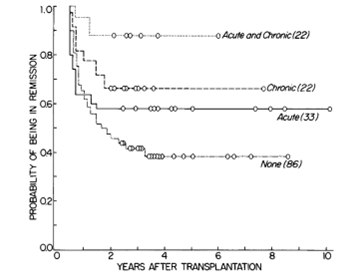
Hope:
2 pivotal publications from 1979 and 1981 in @NEJM described powerful graft-versus- leukemia effects associated with acute and chronic GVHD, providing the rationale for the subsequent introduction of donor lymphocyte infusions in the 1990s.
Hope:
2 pivotal publications from 1979 and 1981 in @NEJM described powerful graft-versus- leukemia effects associated with acute and chronic GVHD, providing the rationale for the subsequent introduction of donor lymphocyte infusions in the 1990s.
16/
Let's recap what we've seen after great disappointment but resilience of the few to improve BMT from the 70s.
Let's recap what we've seen after great disappointment but resilience of the few to improve BMT from the 70s.
17/
To the mountain top, together:
One limitation in early BMT was access, only 35% had HLA-identical siblings
👉registries were built @AnthonyNolan @BeTheMatch @DKMS_de etc.
To the mountain top, together:
One limitation in early BMT was access, only 35% had HLA-identical siblings
👉registries were built @AnthonyNolan @BeTheMatch @DKMS_de etc.

18/
Love:
Nothing is worthwhile when you do it alone. Gösta Gahrton (a European BMT pioneer) told me, BMT without Donnall AND Dotti Thomas wouldn’t exist as is. He remarked that if Donnall Thomas was considered the father of BMT, "then Dottie Thomas was the mother".
Love:
Nothing is worthwhile when you do it alone. Gösta Gahrton (a European BMT pioneer) told me, BMT without Donnall AND Dotti Thomas wouldn’t exist as is. He remarked that if Donnall Thomas was considered the father of BMT, "then Dottie Thomas was the mother".
19/
Reflection:
I was born in 1990 just before his lecture, watched it 1st time few years back, still in awe of the resilience that led us to that point and beyond. I am grateful for this spirit of science and medicine.
Lecture👉 nobelprize.org/prizes/medicin…
Reflection:
I was born in 1990 just before his lecture, watched it 1st time few years back, still in awe of the resilience that led us to that point and beyond. I am grateful for this spirit of science and medicine.
Lecture👉 nobelprize.org/prizes/medicin…
20/
Fin:
The beauty of BMT is what I call “interventional humanism”. No allogeneic BMT without a donor, without registries and societies like @TheEBMT @CIBMTR @ASTCT @BeTheMatch @WMDA_office @ASH_hematology @EHA_Hematology... We cant exist alone, let's work together, 1 world!
Fin:
The beauty of BMT is what I call “interventional humanism”. No allogeneic BMT without a donor, without registries and societies like @TheEBMT @CIBMTR @ASTCT @BeTheMatch @WMDA_office @ASH_hematology @EHA_Hematology... We cant exist alone, let's work together, 1 world!
Some helpful sources:
science-connections.com/books/other/ra…
ncbi.nlm.nih.gov/pmc/articles/P…
Archives of NEJM, esp BMT 2 parts by D. Thomas et al. 1975
ncbi.nlm.nih.gov/pmc/articles/P…
aacrjournals.org/cancerres/arti…
science-connections.com/books/other/ra…
ncbi.nlm.nih.gov/pmc/articles/P…
Archives of NEJM, esp BMT 2 parts by D. Thomas et al. 1975
ncbi.nlm.nih.gov/pmc/articles/P…
aacrjournals.org/cancerres/arti…
• • •
Missing some Tweet in this thread? You can try to
force a refresh